It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

Corona Virus Updates Part 6
page: 56share:
a reply to: pasiphae
The infection is all through society, and the serological tests are showing that. The infection is wide, but the deaths are few. We are watching the herd immunity in action. Those with poor immune systems die, those with good immune systems survive and become immunized. Everybody is starting to understand that it seems.
The infection is all through society, and the serological tests are showing that. The infection is wide, but the deaths are few. We are watching the herd immunity in action. Those with poor immune systems die, those with good immune systems survive and become immunized. Everybody is starting to understand that it seems.
I think you are jumping to conclusions, some of which may be unwarranted. Infection rates vary a lot by region, but this immunity claim of yours is not so certain and more research is needed.
originally posted by: Salander
a reply to: pasiphae
The infection is all through society, and the serological tests are showing that. The infection is wide, but the deaths are few. We are watching the herd immunity in action. Those with poor immune systems die, those with good immune systems survive and become immunized. Everybody is starting to understand that it seems.
C oronavirus Can Be Reactivated After COVID-19 Patients Survived; Second Time Can Be Fatal
That's a potential concern which I don't think is proven yet. The virus is still not well understood and more research is needed.
There is one problem, above most, that is particularly alarming. It's that if you are healed from the virus, it doesn't give you immunity over it, which is widely believed to be the case that when you are done having the coronavirus and is cured your body will be immune to it, granted the virus doesn't mutate too much.
Can You Develop COVID-19 Twice? Here’s What We Know
So let's not assume we know the answer before the research is completed and before we understand what's happening, I think we aren't sure yet.
The World Health Organization (WHO) says we don’t have enough evidence to understand if and why some people may experience reactivation after recovery.
It’ll take time, and a lot of research, before we have a clear picture of the virus’s behavior.
“The truth is that we don’t exactly understand the dynamics of how people who test negative after initial infection end up testing positive again. We need more studies to clarify this observed phenomenon,” says Dr. Robert Glatter, an emergency physician at Lenox Hill Hospital in New York City.
Some doctors treating the virus streamed their conference discussing their treatments and the doctor in Brooklyn says it's not like what they've been trained to treat and it's not the same in all patients, so treatments must be tailored to the individuals. These doctors on the front line still don't understand exactly what the virus is doing, and it sounds like there is some trial and error to see what works and what doesn't:
That was very educational, thank you.
originally posted by: puzzled2
from a week ago
but the did say they are trying everything and running short and out of lots of stuff but look for "Adult tummy time"
to become a trending topic in breathing.
Some medical terminology I was unfamiliar with, like the patients categorized as "LLS", and how they could go from not LLS to LLS and back to not LLS rather quickly. Actually I don't think that's official medical terminology, but they use it.
I would like to know more about this "DDDS", or "Don't So Dumb #", that Laura mentioned. She didn't name names or exact "dumb #" but she obviously had some concerns that some doctors were going off the rails a bit in their exasperation to find successful treatments.
One thing I found especially interesting related to PPE. Remember Americans were told they didn't need to wear masks in an effort to save the N95 masks for the medical folks who needed them? According to these doctors, they consider anything less than PAPR (Powered air-purifying respirator) to be inadequate protection. This is what PAPR looks like, nothing like an N95 mask:
Powered air-purifying respirator

So much for saving the N95 masks for doctors; they want PAPRs, not N95 masks.
edit on 2020424 by Arbitrageur because: clarification
a reply to: Byrd
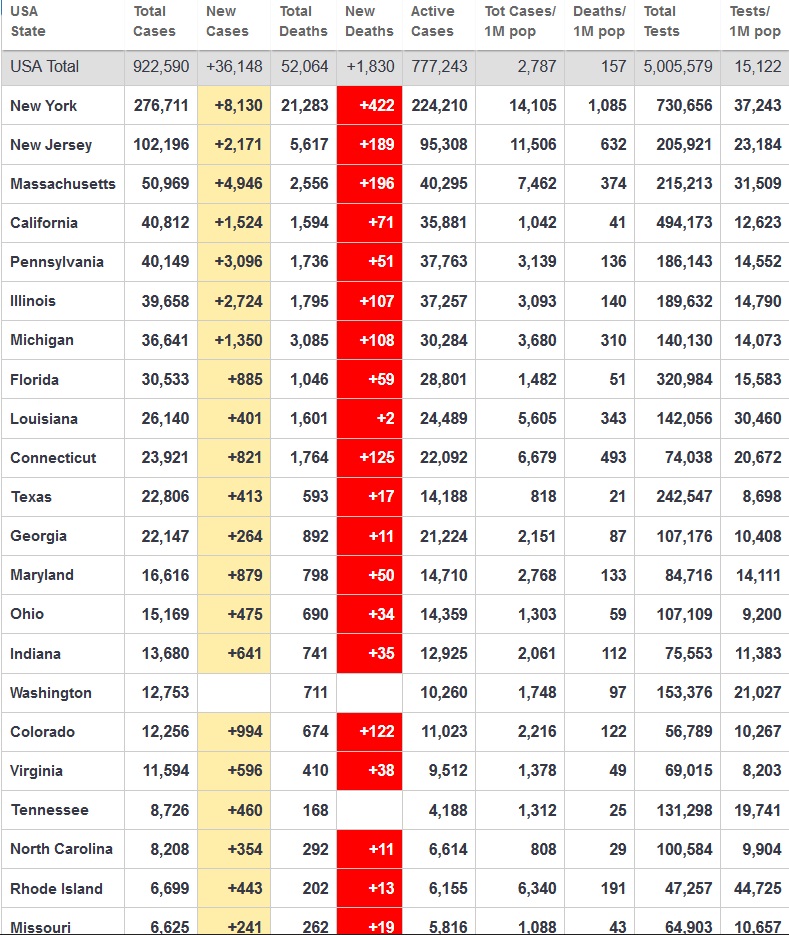
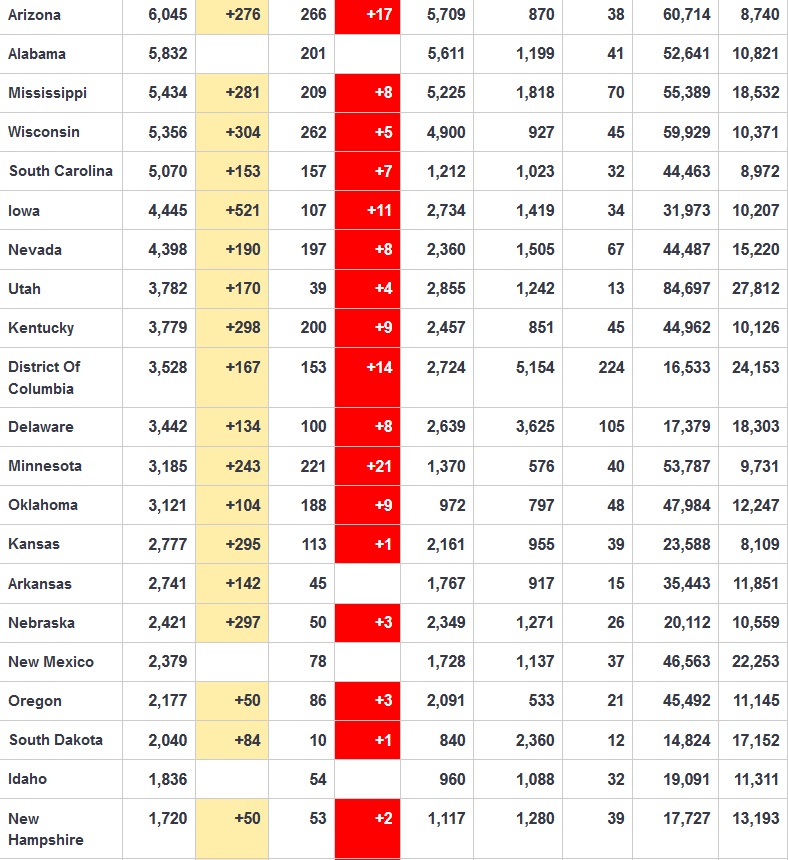
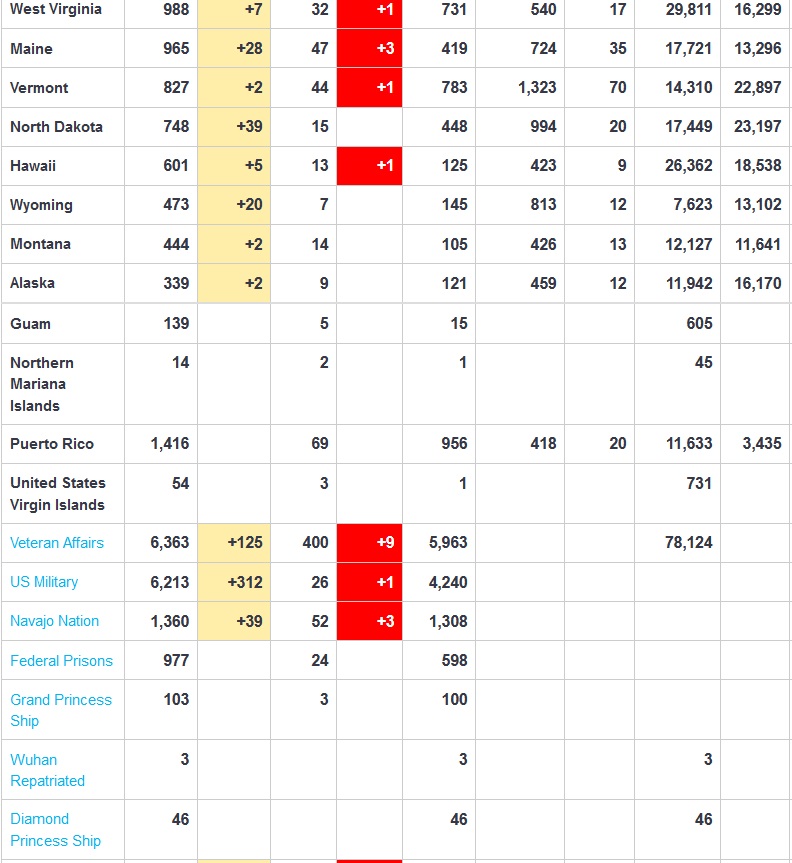
That's my initial instinct too Byrd. I've been scouring the nys health department website for RAW numbers, not the public facing type stuff. So far this is about as far as i can get however, it conspicuously leaves out hospitalization rates.
What I fear about this, is that the numbers are being "flattened" to foster an environment ideally suited to talks about re-opening prematurely. Also, Cuomo taken as a whole has been very quick to call ideas from a guy like McConnell as "dumb" but bends over for Trump's rhetoric.... (which at least I can hope we all agree that rhetoric like injecting disinfectants is NOT a great idea...) which raises an eyebrow for me.
That's my initial instinct too Byrd. I've been scouring the nys health department website for RAW numbers, not the public facing type stuff. So far this is about as far as i can get however, it conspicuously leaves out hospitalization rates.
What I fear about this, is that the numbers are being "flattened" to foster an environment ideally suited to talks about re-opening prematurely. Also, Cuomo taken as a whole has been very quick to call ideas from a guy like McConnell as "dumb" but bends over for Trump's rhetoric.... (which at least I can hope we all agree that rhetoric like injecting disinfectants is NOT a great idea...) which raises an eyebrow for me.
originally posted by: Byrd
originally posted by: alphabetaone
a reply to: Byrd
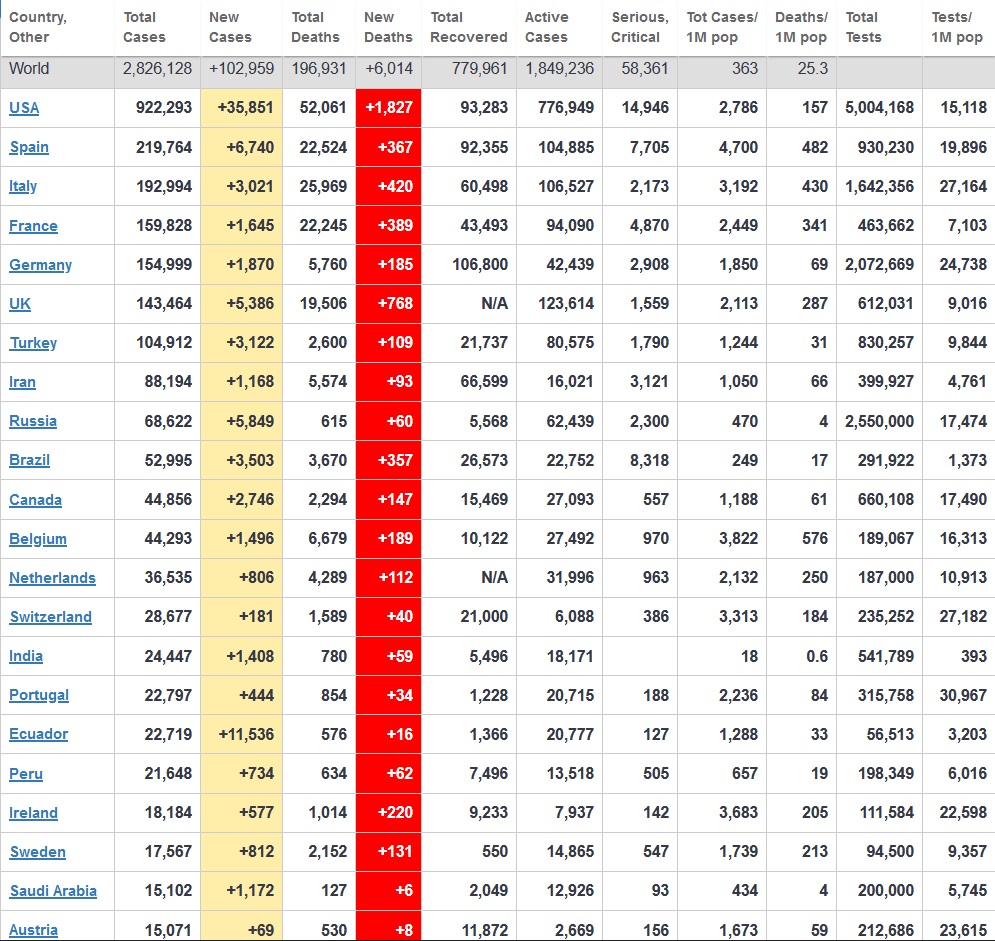
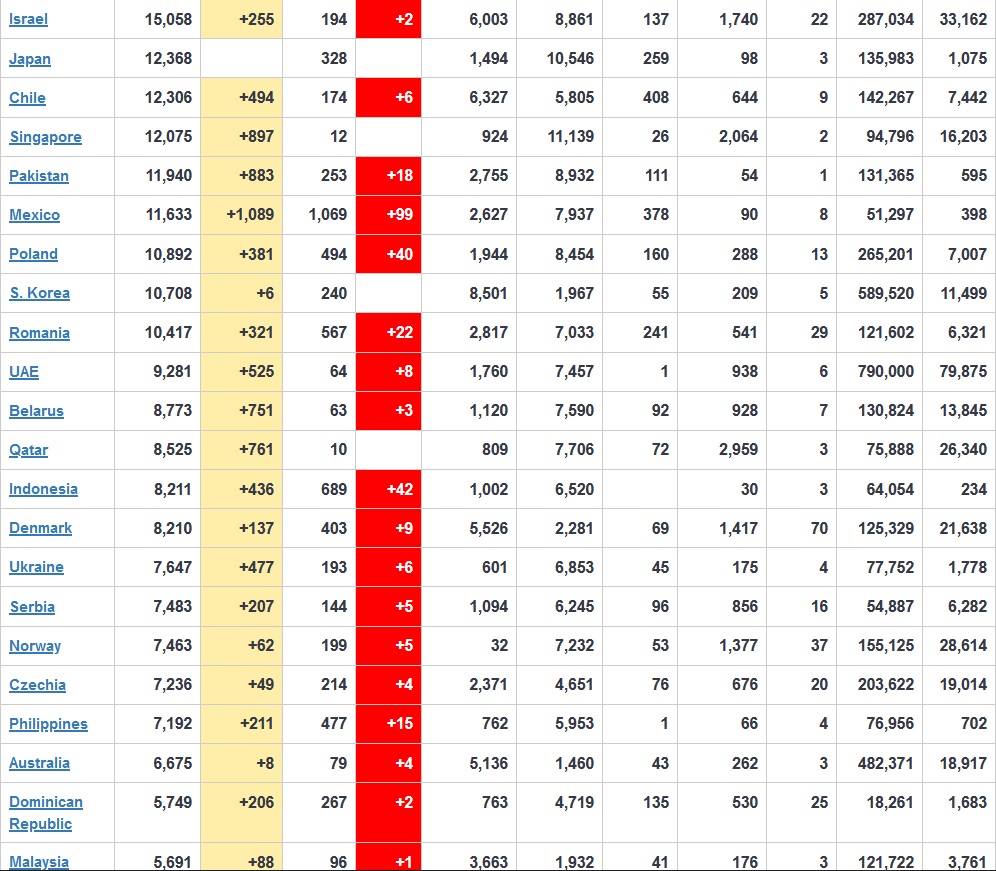
Regrettably this is from "the" definitive source. John Hopkins University. Everyone is basing their numbers (and rises/plateaus/declines) it seems on their collaborative. Im not sure there's a more comprehensive set of data out there. If so though, I would love to see it.
Johns Hopkins is getting numbers from state health departments (they have to get it from somewhere reliable....) So I'm thinking you've got data that's not being updated.
But do check local and state resources. Although Johns Hopkins doesn't report on it, the Texas Tribune does give hospitalizations for Texas: www.texastribune.org... So you might be able to find a secondary source somewhere.
Wikipedia has some of the numbers you're looking for. Hold your mouse over the different parts of the bar charts here: en.wikipedia.org...(state)
New York State and City
Is a site I’ve been going to for state and city info. Hospitalization total has been trending steadily downward which lines with what Cuomo has been saying at briefings - More daily discharge than admissions lately.
I guess now you can find out cases and death by the city by using the zip codes. Pretty cool. Just found that out this morning.
My hometown by using the zip code reveals this:
Positive cases 84 ( my daughter and her family and also my family lives in this town )
Deaths N/A ( I wonder why that is) ?
Tested 213 ( I simply can't believe that, is that really true across America also in small towns )
The above is a city in the Quad Cities in Illinois
So how does one get tested in a small city?
This is the link for Illinois: dph.illinois.gov...
My hometown by using the zip code reveals this:
Positive cases 84 ( my daughter and her family and also my family lives in this town )
Deaths N/A ( I wonder why that is) ?
Tested 213 ( I simply can't believe that, is that really true across America also in small towns )
The above is a city in the Quad Cities in Illinois
So how does one get tested in a small city?
This is the link for Illinois: dph.illinois.gov...

a reply to: Arbitrageur
Kudos to you for that post.
I don't usually (ever?) just post to say : good job, but actually, GOOD JOB.
Your post is exactly consistent with what myself and the people with whom I work are seeing.
We all are learning as we go along. Truly.
Thanks.
Sorry that I don't have so much time to add to this, but thanks.
What you have just posted is consistent with my own (limited) experience.
Kudos to you for that post.
I don't usually (ever?) just post to say : good job, but actually, GOOD JOB.
Your post is exactly consistent with what myself and the people with whom I work are seeing.
We all are learning as we go along. Truly.
Thanks.
Sorry that I don't have so much time to add to this, but thanks.
What you have just posted is consistent with my own (limited) experience.
originally posted by: musicismagic
I guess now you can find out cases and death by the city by using the zip codes. Pretty cool. Just found that out this morning.
I didn't know that was available. Went out and looked for Dallas county just now and found it. Mine only shows confirmed cases.
My hometown by using the zip code reveals this:
Positive cases 84 ( my daughter and her family and also my family lives in this town )
Deaths N/A ( I wonder why that is) ?
Tested 213 ( I simply can't believe that, is that really true across America also in small towns )
I can believe it. They probably only test at hospitals and only if someone's sick enough to go there.
originally posted by: Byrd
Last paragraph in this article, which says he only treated 14 patients and that the community has asked him to quit making these false claims.
Ummm... no, he only tested 14 patients. There is a difference.
3 confirmed and 2 probable cases in Aotearoa/New Zealand today all linked to known clusters. Going down to alert level three on monday 11.59pm, could
have made it earlier but ANZAC day holiday on the monday so a long weekend is not a good idea as people want to pop their bubbles and go away or
visit family hence the longer level four lockdown.
Personally on ANZAC day I like to remember all the innocent people who died in the war, not just the killers.
Personally on ANZAC day I like to remember all the innocent people who died in the war, not just the killers.
I'm not used to giving or receiving that kind of feedback so thanks for the feedback.
originally posted by: Fowlerstoad
a reply to: Arbitrageur
Kudos to you for that post.
I don't usually (ever?) just post to say : good job, but actually, GOOD JOB.
One other thing I thought was interesting in the doctors' conference; the doctor in Brooklyn was using a "high flow" oxygen treatment on some patients. Apparently "high flow" is aptly named, because he said it will run through one of those giant oxygen tanks in about 90 minutes. Not one of those smaller oxygen tanks some people might have seen, the really big ones. So he said keeping enough oxygen tanks around can be a challenge when he has multiple patients going through a large tank every 90 minutes EACH!
The doctor in Italy said they don't have many high flow systems at their hospital so they don't have much option to use it for treatment at present. They are trying to use more CPAP and less ventilators. This discusses the non-invasive alternatives to intubation of the high-flow and CPAP:
COVID-19: Alternatives to ventilators
Understanding which ventilation technique is appropriate for each patient can help improve patient care and assist clinical teams for success. There are different ways to support COVID-19 patients with NIV therapy and depending on the route of the best course of treatment, each comes with different considerations. Below are the most common NIV therapies, with recommendations on how the transmission risk can be reduced:
High-Flow Nasal Cannula (HFNC): If oxygen delivered via HFNC is an option for patients with mild hypoxemic respiratory failure:
o Provide masks to be worn over the nasal cannula to reduce the potential for airborne virus transmission.
o Ensure timely endotracheal intubation and positive pressure mechanical ventilation if the patient’s clinical status deteriorates [3-4].
Continuous Positive Airway Pressure (CPAP) or Bilevel Positive Airway Pressure (BiPAP): If CPAP or BiPAP is considered appropriate in patients with mild hypoxemia and hypercarbia – such as patients with exacerbation of chronic obstructive pulmonary disease (COPD):
o Use a well-fitted oro-nasal mask (or helmet, if available). Avoid use of nasal masks and/or nasal pillows, if possible.
o Employ a dual-limb ventilator with filters placed at the ventilator outlets.
o Using an appropriate and compatible expiratory port filter for single-limb non-invasive ventilators will reduce the risk of virus spread in the open patient room [5].
Of course, vigilance is required to ensure timely endotracheal intubation and positive pressure ventilation if a patient’s clinical status deteriorates.
There is another issue hospitals with a lot of patients are having problems with. Even these non-invasive alternatives to ventilators require constant monitoring of the patients as their condition can deteriorate quickly in which case their treatment may need to be changed; maybe they will need the invasive ventilator if that happens. But the inundated hospital in Brooklyn and presumably others only have continuous monitoring of patients in ICU and the emergency room areas, so it's a problem that moving patients to other beds in the hospital means they won't get monitored, and there aren't enough beds in ICU and the ER so they are having to improvise some solutions to keep the patients monitored.
Also apparently those alternatives to ventilators cause more aerosolization of the virus which is one reason the doctors using them need extremely robust personal protective equipment to use them, like the PPAP. Masks aren't good enough.
This virus seems challenging in many ways, to not only slow the spread, but to figure out ways to treat people who are symptomatic.
edit on 2020424 by Arbitrageur because: clarification
Don't live in NY so not sure of the areas.
Wondering if there is any coloration between the big weddings and gatherings that were going on and cases in hospitals?
Examples New Jersey cops break up two large weddings amid coronavirus restrictions
if there has been a large gathering did anyone get anmes to cross reference a clusterf# that can be identified or has there been no cluster and the people are - lucky no-one had it, or all got it but no hospitalization.
In terms of updates how could we verify R0 values
Wondering if there is any coloration between the big weddings and gatherings that were going on and cases in hospitals?
Examples New Jersey cops break up two large weddings amid coronavirus restrictions
if there has been a large gathering did anyone get anmes to cross reference a clusterf# that can be identified or has there been no cluster and the people are - lucky no-one had it, or all got it but no hospitalization.
In terms of updates how could we verify R0 values
Letter to the editor Covid-19 and New Onset Arrythmia
A finding from a hospital. This is in the form of a "letter to the editor" which means they think it's important but they don't have time to do formal research.
So the basics here are that they first acknowledge some of the emerging reports...that in the case of Covid-19 deaths, a significant number (reports indicate 20% or more) die from a heart injury that causes the heartbeat to go haywire. They feel the evidence points to the cytokene storm doing some sort of hyper-inflammation to the heart which causes the beat to go bonkers.
They note that this kind of response is actually fairly common with viral infections and say that managing the infection response should reduce the number of arrhythmia deaths. They note one drug trial (the implication is that this is a drug trial to watch.)
A finding from a hospital. This is in the form of a "letter to the editor" which means they think it's important but they don't have time to do formal research.
So the basics here are that they first acknowledge some of the emerging reports...that in the case of Covid-19 deaths, a significant number (reports indicate 20% or more) die from a heart injury that causes the heartbeat to go haywire. They feel the evidence points to the cytokene storm doing some sort of hyper-inflammation to the heart which causes the beat to go bonkers.
They note that this kind of response is actually fairly common with viral infections and say that managing the infection response should reduce the number of arrhythmia deaths. They note one drug trial (the implication is that this is a drug trial to watch.)
a reply to: Byrd
What I find interesting iis that Australia and New Zealand have up to a 50% higher UV value than everywhere else in the world.
I've been wondering what makes Aus and NZ special... because we are actually crap at social distancing...
Is it as simple as high UV?
What I find interesting iis that Australia and New Zealand have up to a 50% higher UV value than everywhere else in the world.
I've been wondering what makes Aus and NZ special... because we are actually crap at social distancing...
Is it as simple as high UV?
a reply to: puzzlesphere
OR Editorial: low population mortality from COVID‐19 in countries south of latitude 35 degrees North – supports vitamin D as a factor determining severity
They have high sunbathing and the imported victims didn't have the time to get enough Vit D.
There was a lot of talk in the beginning giving vit D and C is it still happening in the high death regions?
OR Editorial: low population mortality from COVID‐19 in countries south of latitude 35 degrees North – supports vitamin D as a factor determining severity
They have high sunbathing and the imported victims didn't have the time to get enough Vit D.
There was a lot of talk in the beginning giving vit D and C is it still happening in the high death regions?
a reply to: puzzled2
I think the graphs in this vid which I posted on another forum , shows how the flue gains when the populations vitamin D levels drop during winter. Remembering we are also going into a solar minimum, plus people using sun block just blocks the wrong rays, to the extent the people who wear no sunblock have a much lower Skin cancer risk than the people that use it all the time. Its one of the best Vids with all the latest data, which proves that recommended doses of Vitamin D are far to low and their is no real toxic limit. The fact that at present most people in the higher latitudes are in the danger zones with regards to this is the most concerning thing I have seen for years.
I think the graphs in this vid which I posted on another forum , shows how the flue gains when the populations vitamin D levels drop during winter. Remembering we are also going into a solar minimum, plus people using sun block just blocks the wrong rays, to the extent the people who wear no sunblock have a much lower Skin cancer risk than the people that use it all the time. Its one of the best Vids with all the latest data, which proves that recommended doses of Vitamin D are far to low and their is no real toxic limit. The fact that at present most people in the higher latitudes are in the danger zones with regards to this is the most concerning thing I have seen for years.
originally posted by: puzzlesphere
a reply to: Byrd
What I find interesting iis that Australia and New Zealand have up to a 50% higher UV value than everywhere else in the world.
I've been wondering what makes Aus and NZ special... because we are actually crap at social distancing...
Is it as simple as high UV?
Don't know where you got the "UV value"... UV index, perhaps? If it's UV index, the highest values were actually measured in South America... which has a really disastrous rate (where it's measured.) Here in the US, Texas and New Mexico and Arizona and southern California all have lots of pure sunshine, and I can assure you that we're seeing low values because there's a low population density. If you look at Egypt and Saudi Arabia (etc) you will see no protective effect.
What would help:
* good health system
* people NOT living in multifamily groups inside a single small building
* economic stability
* first world country/high standard of living
...and a population with few health problems and not many old people.
If all those conditions are satisfied and the people aren't cooped up in offices, breathing and re-breathing the same air, then we would probably see a small positive impact in warmer climates.
IMHO, of course.
Rather than overwhelm the thread with half a dozen posts, I'm going to lump a few together.
FIRST ARTICLE
From the very prestigious (and very very very hard to have a paper accepted... I know this from personal experience) Journal of the American Medical Association (JAMA)
Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility
This is a horrifying article, particularly if you know (as I do) one or more people in a nursing home/living facility. They tested people in a nursing home when the first case of Covid-19 showed up and then tested everyone a week later.
So it gallops through a facility (any facility where people are in contact with each other for many hours a day) and you can quickly reach 60%+ infection rate.
NOTE: This is a featured article, not a stable URL. If you see this post sometime after May 5, 2020, it may not be at this link.
SECOND ARTICLE
UCHICAGO Doctors See truly remarkable success using ventilator alternatives I think this may have been posted (or a news report about it)... basically they're using nasal canula which is a lot less invasive than the respirators.
NEWS ARTICLE
Africa Dangerously Behind in race for Virus Gear I'd mentioned this .... many many messages ago in a long-forgotten post that Africa could become a reservoir because of poor access to medical equipment and resources to fight the virus. This article goes into it in some depth.
SECOND ARTICLE
Cities, Crowding, and Coronavirus = Predicting Contagion Risk Hotspots
This is a great blog post and some very basic science on why we see hotspots in some areas but in many areas there's nobody in the hospital with Covid-19.
To quote from one paragraph:
Really worth a read. Not very long blog post.
FIRST ARTICLE
From the very prestigious (and very very very hard to have a paper accepted... I know this from personal experience) Journal of the American Medical Association (JAMA)
Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility
This is a horrifying article, particularly if you know (as I do) one or more people in a nursing home/living facility. They tested people in a nursing home when the first case of Covid-19 showed up and then tested everyone a week later.
Twenty-three days after the first positive test result in a resident at this skilled nursing facility, 57 of 89 residents (64%) tested positive for SARS-CoV-2. Among 76 residents who participated in point-prevalence surveys, 48 (63%) tested positive. Of these 48 residents, 27 (56%) were asymptomatic at the time of testing; 24 subsequently developed symptoms (median time to onset, 4 days)
So it gallops through a facility (any facility where people are in contact with each other for many hours a day) and you can quickly reach 60%+ infection rate.
NOTE: This is a featured article, not a stable URL. If you see this post sometime after May 5, 2020, it may not be at this link.
SECOND ARTICLE
UCHICAGO Doctors See truly remarkable success using ventilator alternatives I think this may have been posted (or a news report about it)... basically they're using nasal canula which is a lot less invasive than the respirators.
NEWS ARTICLE
Africa Dangerously Behind in race for Virus Gear I'd mentioned this .... many many messages ago in a long-forgotten post that Africa could become a reservoir because of poor access to medical equipment and resources to fight the virus. This article goes into it in some depth.
SECOND ARTICLE
Cities, Crowding, and Coronavirus = Predicting Contagion Risk Hotspots
This is a great blog post and some very basic science on why we see hotspots in some areas but in many areas there's nobody in the hospital with Covid-19.
To quote from one paragraph:
But poorer residents of crowded neighborhoods cannot afford such luxuries. They are forced to leave their home every day to go to work, buy groceries, and do laundry. This is especially true in low-income neighborhoods of developing countries – many of which are slums and informal settlements. Here many residents live in substandard housing and overcrowded conditions. The lack of adequate infrastructure means that they share taps and latrines, with as many as 200 people per communal facility. Most people living in these communities are daily wage earners in the informal sector, with irregular income and insecure jobs. They cannot realistically practice social distancing, nor can they afford it.
Really worth a read. Not very long blog post.
edit on 25-4-2020 by Byrd because: (no reason given)
new topics
-
The Mystery Drones and Government Lies
Other Current Events: 24 minutes ago -
Pelosi injured in Luxembourg
Other Current Events: 7 hours ago -
Nov 2024 - Former President Barack Hussein Obama Has Lost His Aura.
US Political Madness: 8 hours ago
top topics
-
Pelosi injured in Luxembourg
Other Current Events: 7 hours ago, 12 flags -
Something better
Dissecting Disinformation: 14 hours ago, 8 flags -
Nov 2024 - Former President Barack Hussein Obama Has Lost His Aura.
US Political Madness: 8 hours ago, 7 flags -
More Ons?
Political Conspiracies: 17 hours ago, 6 flags -
Friday thoughts
General Chit Chat: 17 hours ago, 5 flags -
Canada Post strike ended by the Government of Canada
Mainstream News: 17 hours ago, 4 flags -
The Witcher IV — Cinematic Reveal Trailer | The Game Awards 2024
Video Games: 16 hours ago, 3 flags -
The Mystery Drones and Government Lies
Other Current Events: 24 minutes ago, 1 flags
active topics
-
The Mystery Drones and Government Lies
Other Current Events • 1 • : chiefsmom -
A Bunch of Maybe Drones Just Flew Across Hillsborough County
Aircraft Projects • 74 • : anned1 -
Pelosi injured in Luxembourg
Other Current Events • 17 • : chiefsmom -
Magic Vaporizing Ray Gun Claim - More Proof You Can't Believe Anything Hamas Says
War On Terrorism • 21 • : FlyersFan -
What Am I Hearing
General Chit Chat • 13 • : charlest2 -
One out of every 20 Canadians Dies by Euthanasia
Medical Issues & Conspiracies • 20 • : DISRAELI2 -
Something better
Dissecting Disinformation • 19 • : GENERAL EYES -
They Know
Aliens and UFOs • 76 • : Kangawoo2 -
Drones everywhere in New Jersey
Aliens and UFOs • 113 • : WeMustCare -
Top Sci Fi/Horror Crossover Movies
Movies • 14 • : GotterDameron23