It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

Ebola: Facts, Opinions, and Speculations.
page: 24share:
Um...
Does this patient have Ebola virus disease?
Anyone have academic access and can pull the contents?
This has been tweeted 3x as seen here.
Does this patient have Ebola virus disease?
Title
Does this patient have Ebola virus disease?
Journal
Intensive Care Medicine
DOI10.1007/s00134-014-3473-7
Print ISSN0342-4642
Online ISSN1432-1238
PublisherSpringer Berlin Heidelberg
Anyone have academic access and can pull the contents?
edit on 6-9-2014 by jadedANDcynical because: (no reason given)
This has been tweeted 3x as seen here.
edit on 6-9-2014 by jadedANDcynical
because: (no reason given)
Again, so people stop confusing them:
Case Fatality Rate = 100 people get Ebola, 50 people die, Case Fatality Rate 50%
That is not to be confused with
Mortality Rate = 1,000 people live in XXX, 100 people get Ebola, 50 people die, Mortality Rate 5%
People are using Mortality Rate where they should be using Case Fatality Rate.
Case Fatality Rate = 100 people get Ebola, 50 people die, Case Fatality Rate 50%
That is not to be confused with
Mortality Rate = 1,000 people live in XXX, 100 people get Ebola, 50 people die, Mortality Rate 5%
People are using Mortality Rate where they should be using Case Fatality Rate.
originally posted by: soficrow
a reply to: ikonoklast
....But. Fact is, there is NO WAY to seal off Guinea, Liberia, and Sierra Leone. And is there any reason to believe Ebola respects political borders? ....What are the chances it's already raging through Mali and Cote d'Ivoire - but not being reported?
PS. An earlier report said infections were doubling every 34.8 days. My calculations say it's now increasing by 2.3 every month. What's your infection rate number? Do you see an increased rate of infection?
True, there is no way to seal off these countries. But I think TPTB have concluded containment is the only possible solution. Personally, I think it is likely there are already cases in other countries that are not being reported or that perhaps have not been identified.
I put together a draft of a chart showing how the doubling rate has varied over time. The y-axis shows how many days it took for cases to double for any given date on the x-axis.
For those taking a quick glance, remember that on this chart, high spikes are good, low spikes are bad. Click on the graphic to see it full-size:
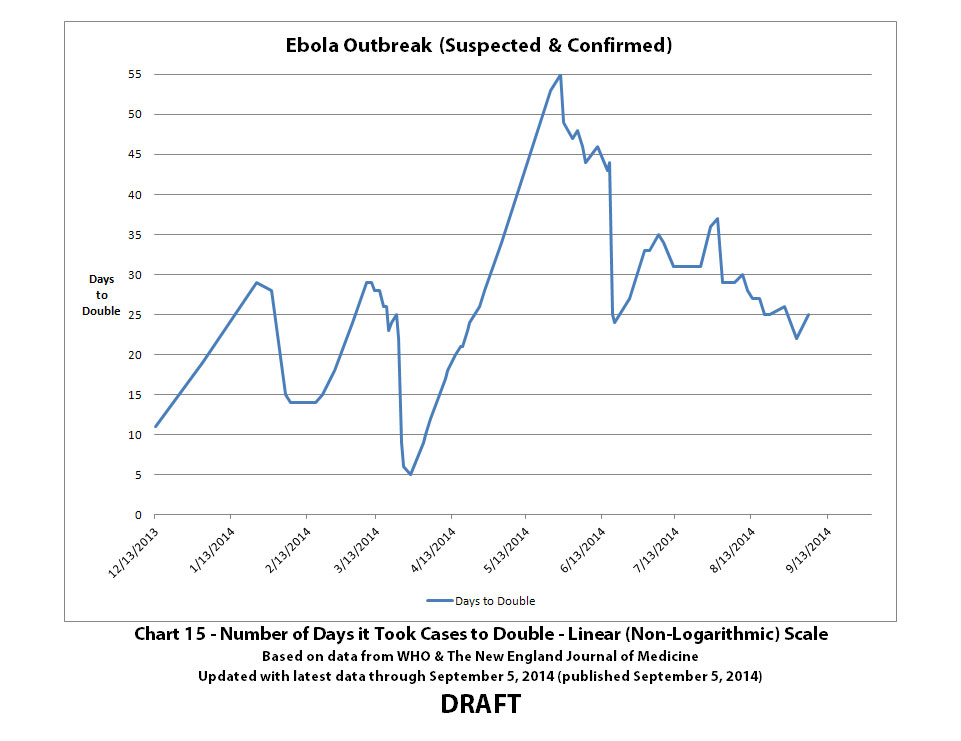
Some things to bear in mind:
The first known case became symptomatic on December 2, 2013, so when the chart show 11 days to double on December 13, 2013, that's the first case doubling to 2 cases. Definitely not a very big data sample. The data sample may not be big enough to conclude much from it for days prior to June or July 2014.
WHO realized there was an Ebola outbreak on or about March 22, 2014, and that's when they began tracking it. So the drop in number of days it took for cases to double around that time may or may not be partly related to more cases being recognized as Ebola.
I read somewhere that WHO thought that this Ebola outbreak would naturally decline like previous outbreaks back in May 2014. It's easy to see why looking at this graph. Unfortunately, things went the other way.
a reply to: ikonoklast
Doctors Without Borders (MSF) was in the field at/near the epicenter from January-February - the epicenter being the area where the borders of Sierra Leone, Guinea and Liberia all meet. MSF was treating patients from Sierra Leone and Liberia, not just Guinea. However, only Guinea chose to report their Ebola cases to the WHO - Sierra Leone and Liberia both denied Ebola's presence in their countries. As you know, the WHO is in a tricky political position and cannot document cases unless nations release reports. In addition, previous outbreaks remained isolated and "burned out" before spreading - the (off site) "experts" assumed the same would happen despite warnings to the contrary from MSF in the field - and besides, the WHO's budget had been slashed so they didn't have either the resources or mandate. By March, MSF called "Ebola Epidemic" saying it "could become a global crisis" at that time. ....It was 2 months before people started listening, and 3 months before any action was taken. Sierra Leone and Liberia did not start reporting til when? June? During that delay the ISIS crisis ...evolved. We're still waiting for concerted appropriate action on the Ebola epidemic.
Sorry. Had to say it.
...I read somewhere that WHO thought that this Ebola outbreak would naturally decline like previous outbreaks back in May 2014. It's easy to see why looking at this graph. Unfortunately, things went the other way.
Doctors Without Borders (MSF) was in the field at/near the epicenter from January-February - the epicenter being the area where the borders of Sierra Leone, Guinea and Liberia all meet. MSF was treating patients from Sierra Leone and Liberia, not just Guinea. However, only Guinea chose to report their Ebola cases to the WHO - Sierra Leone and Liberia both denied Ebola's presence in their countries. As you know, the WHO is in a tricky political position and cannot document cases unless nations release reports. In addition, previous outbreaks remained isolated and "burned out" before spreading - the (off site) "experts" assumed the same would happen despite warnings to the contrary from MSF in the field - and besides, the WHO's budget had been slashed so they didn't have either the resources or mandate. By March, MSF called "Ebola Epidemic" saying it "could become a global crisis" at that time. ....It was 2 months before people started listening, and 3 months before any action was taken. Sierra Leone and Liberia did not start reporting til when? June? During that delay the ISIS crisis ...evolved. We're still waiting for concerted appropriate action on the Ebola epidemic.
Sorry. Had to say it.
originally posted by: soficrow
a reply to: ikonoklast
...I read somewhere that WHO thought that this Ebola outbreak would naturally decline like previous outbreaks back in May 2014. It's easy to see why looking at this graph. Unfortunately, things went the other way.
[snip]
In addition, previous outbreaks remained isolated and "burned out" before spreading - the (off site) "experts" assumed the same would happen despite warnings to the contrary from MSF in the field
[snip]
Taking off on a tangent on what you said, it brings up a good point. The official western reaction for the former outbreaks of Ebola were just to let them burn themselves out. Now the truth comes out.
All this time since the outbreaks in the 90s and later, I thought that somehow the doctors that went there were some kinds of heroes to stop Ebola. What a wonderful feat! Then it turns out that really it seems that they did very little, and really the Ebola just stopped on its own. hhhhhmmmm... interesting.
originally posted by: MarkJS
originally posted by: soficrow
a reply to: ikonoklast
...I read somewhere that WHO thought that this Ebola outbreak would naturally decline like previous outbreaks back in May 2014. It's easy to see why looking at this graph. Unfortunately, things went the other way.
[snip]
In addition, previous outbreaks remained isolated and "burned out" before spreading - the (off site) "experts" assumed the same would happen despite warnings to the contrary from MSF in the field
[snip]
....All this time since the outbreaks in the 90s and later, I thought that somehow the doctors that went there were some kinds of heroes to stop Ebola. What a wonderful feat! Then it turns out that really it seems that they did very little, and really the Ebola just stopped on its own. hhhhhmmmm... interesting.
Not sure what you're getting at but it has been observed and is an accepted fact that historically, Ebola outbreaks remain geographically isolated and burn themselves out within a matter of months. The work done by hero-doctors is important either way - patients suffer and need care even when they're dying, and sometimes that care means the difference between life and death.
a reply to: MarkJS
Wow. Just because the doctors are waiting for it to burn out doesn't make them heroes?? They are there at the risk of their own lives to help those who are dying, and to try and prevent the spread of the disease. It is their work that usually helps it burn out so quickly. They also directly help people survive the disease who would not otherwise.
Wow. Just because the doctors are waiting for it to burn out doesn't make them heroes?? They are there at the risk of their own lives to help those who are dying, and to try and prevent the spread of the disease. It is their work that usually helps it burn out so quickly. They also directly help people survive the disease who would not otherwise.
a reply to: raymundoko
What are yor medical qualifications and how many publications have you authored?
Here are some of hers in addition to the one I referenced im the post t which yours replies to.
This is the department she works in:
I think she is more than "only a nurse." The document in question appears to be a training presentation only recently authored. I think it highly unlikely that she would make such a mistake in a presentation given to the type of audience she writes for. Don't you think it possible that she might be privvy to information not in the general ken?
So far, all I have received is an out of office reply in response to my query.
What are yor medical qualifications and how many publications have you authored?
Here are some of hers in addition to the one I referenced im the post t which yours replies to.
This is the department she works in:
Infection Prevention and Control Team
The Infection Prevention and Control team consists of members of staff with a specialist knowledge and training in Infection Prevention and Control in the hospital setting:
Consultant Microbiologist (who acts as the Infection Prevention and Control doctor and directs the activities of the Infection Prevention and Control Nursing Personnel)
Assistant Director of Nursing, Infection Prevention and Control
Clinical Nurse Manager 2
Surveillance Scientist
The Infection Prevention and Control Team meet regularly, often on a daily basis. These individuals are also members of the Infection Prevention and Control Committee. The Infection Prevention and Control Committee is chaired by the deputy General Manager.
I think she is more than "only a nurse." The document in question appears to be a training presentation only recently authored. I think it highly unlikely that she would make such a mistake in a presentation given to the type of audience she writes for. Don't you think it possible that she might be privvy to information not in the general ken?
So far, all I have received is an out of office reply in response to my query.
Here's the latest update I could find in regards to the Nebraska patient...
(CNN) -- Dr. Rick Sacra, an American missionary doctor infected with the deadly Ebola virus, has improved slightly while being treated in Omaha, Nebraska, his wife said.
Source edition.cnn.com...
Hope I did the posting right as well as in right forum.
Cheers
Ektar
(CNN) -- Dr. Rick Sacra, an American missionary doctor infected with the deadly Ebola virus, has improved slightly while being treated in Omaha, Nebraska, his wife said.
Source edition.cnn.com...
Hope I did the posting right as well as in right forum.
Cheers
Ektar
Don't know if this has been posted but... the author of this blog is a 14 year-old scientist, and his work has received international attention and
acclaim from other scientists, especially this post.
A Brief Passage of Time in the Deadly Ebola Virus
Posted by [email protected] 16 April 14
From the WHO:
Another warning about 'aerosol-generating procedures.'
Wait a second, I thought that it could NOT be caught "through inhalation?"
And if it's so hard to catch and easy to kill, why this for cleaning procedures?
Why all the emphasis on making sure to not produce a circumstamce wherein airborne transmission could occur if the virus can NOT be trasmitted via the airborne route?
Interim Infection Prevention and Control Guidance for Care of Patients with Suspected or Confirmed Filovirus Haemorrhagic Fever in Health-Care Settings, with Focus on Ebola
August 2014
September 08, 2014
Canada: Possible Ebola case at Hôpital Notre-Dame
Tick tock
Avoid aerosol-generating procedures if possible. Wear a respirator (FFP2 or EN certified equivalent or US NIOSH-certified N95), if any procedures that stimulate coughing or promote the generation of aerosols (e.g., aerosolized or nebulized medication administration, diagnostic sputum induction, bronchoscopy, airway suctioning, endotracheal intubation, positive pressure ventilation via face mask) is planned to be performed.
Another warning about 'aerosol-generating procedures.'
Activities such as micro-pipetting and centrifugation can mechanically generate fine aerosols that might pose a risk of transmission of infection through inhalation as well as the risk of direct exposure.
Wait a second, I thought that it could NOT be caught "through inhalation?"
And if it's so hard to catch and easy to kill, why this for cleaning procedures?
all emphases mine
¤ Environmental surfaces or objects contaminated with blood, other body fluids, secretions or excretions should be cleaned and disinfected as soon as possible using standard hospital detergents/disinfectants (e.g. a 0.5% chlorine solution or a solution containing 1 000 ppm available free chlorine)11. Application of disinfectants should be preceded by cleaning to prevent inactivation of disinfectants by organic matter.
¤ If locally prepared, prepare cleaning and disinfectant solutions every day. Change cleaning solutions and refresh equipment frequently while being used during the day, as they will get contaminated quickly (follow your hospital protocols if available). For preparing chlorine-based solutions, see instructions in Annex 6.
¤ Clean floors and horizontal work surfaces at least once a day with clean water and detergent. Cleaning with a moistened cloth helps to avoid contaminating the air and other surfaces with air-borne particles. Allow surfaces to dry naturally before using them again.
¤ Dry sweeping with a broom should never be done. Rags holding dust should not be shaken out and surfaces should not be cleaned with dry rags.
Why all the emphasis on making sure to not produce a circumstamce wherein airborne transmission could occur if the virus can NOT be trasmitted via the airborne route?
Interim Infection Prevention and Control Guidance for Care of Patients with Suspected or Confirmed Filovirus Haemorrhagic Fever in Health-Care Settings, with Focus on Ebola
August 2014
edit on 8-9-2014 by jadedANDcynical because: (no reason given)
A man just arriving from Guinea vomited on the plane Sunday was held in isolation at the Notre Dame Hospital on Sherbrooke Street in Montreal.
Since the patient has visited this country in West Africa where the Ebola virus is prevalent, he was sent directly to Notre Dame, one of two hospitals designated by the Department of Health and Human Services to support patients suspected of carrying Ebola.
September 08, 2014
Canada: Possible Ebola case at Hôpital Notre-Dame
Tick tock
edit on 8-9-2014 by jadedANDcynical because: canada, oh canada
The resurgence of the disease in a place where doctors thought they had it beat shows how history's largest Ebola outbreak has spun out of control.
Read more here: www.newsobserver.com...=cpy
This ebola thing has me on edge. I can't help but think we are in big trouble. I know there are many more widespread diseases than this but this is so deadly. Plus, I don't think anyone knows really what we're dealing with as far as the way it's spread and how many times it's mutated.
a reply to: quirkygirl
i was on edge from the moment i heard about it because ebola had been proposed as a way of killing off 90% of humans by that scientist in a lecture
i was on edge from the moment i heard about it because ebola had been proposed as a way of killing off 90% of humans by that scientist in a lecture
How deadly is Ebola? Statistical
challenges may be inflating survival rate
hope it is 50% rather than 70%
hope it is 50% rather than 70%
edit on 9-9-2014 by joho99 because: (no reason given)
US federal air marshal in quarantine after being stabbed in the arm with a syringe and 'injected with a foreign substance' at Nigerian airport
A U.S. federal air marshal was injected in the back of the arm with an unknown substance at Lagos airport
The assailant has not been located and a motive has not been established
The air marshal was quarantined and screened for Ebola on-scene
He was allowed to board the United Airlines flight he was booked on for Houston
He is having further tests in the United States
The syringe was also transported to the U.S. for testing
Marshal was having symptoms during a flight and he will be tested of Ebola and is quarantined in Houston.
Link
a reply to: joho99
It is even lower if proper medical care is involved. It seems that only 1 out of 5 people who have had PROPER medical care have died. The CFR in the three countries is so high (50-70%) because they have an atrocious medical system.
www.nbcnews.com...
It is even lower if proper medical care is involved. It seems that only 1 out of 5 people who have had PROPER medical care have died. The CFR in the three countries is so high (50-70%) because they have an atrocious medical system.
www.nbcnews.com...
a reply to: jadedANDcynical
Because DUST. Ebola has to have some type of droplet transmission to be spread through the air, and dust is more than capable of carrying Ebola.
Edit: Imagine someone sweating or spitting onto a dusty table (Have you seen the conditions, this is the norm) once the liquid evaporates Ebola is left clinging to dust particles.
Because DUST. Ebola has to have some type of droplet transmission to be spread through the air, and dust is more than capable of carrying Ebola.
Edit: Imagine someone sweating or spitting onto a dusty table (Have you seen the conditions, this is the norm) once the liquid evaporates Ebola is left clinging to dust particles.
edit on 9-9-2014 by raymundoko because: (no reason given)
a reply to: jadedANDcynical
An Aerosol can be many sizes. Droplet transmission is still transmission by aerosols...however Ebola has to be attached to an Aerosol bigger than xx size, making it only communicable via Droplet Transmission and not an Airborne Pathogen.
An Aerosol can be many sizes. Droplet transmission is still transmission by aerosols...however Ebola has to be attached to an Aerosol bigger than xx size, making it only communicable via Droplet Transmission and not an Airborne Pathogen.
a reply to: jadedANDcynical
That is a paper on how to determine if someone may have Ebola without having a test readily available. So the paper is titled with the question: "Does this person have Ebola?".
And from your paper:
It isn't airborne.
That is a paper on how to determine if someone may have Ebola without having a test readily available. So the paper is titled with the question: "Does this person have Ebola?".
And from your paper:
It is transmitted by direct contact through broken skin or mucous membranes with blood, urine, saliva, faeces, vomit, and other body fluids of symptomatic infected patients or convalescent persons, or through contaminated needle sticks
It isn't airborne.
new topics
-
Watching TV
Jokes, Puns, & Pranks: 1 hours ago -
RFK is Trumps health pick
2024 Elections: 9 hours ago
top topics
-
The art of being offended
Social Issues and Civil Unrest: 17 hours ago, 20 flags -
Thanksgiving 2024
Member Art: 15 hours ago, 13 flags -
RFK is Trumps health pick
2024 Elections: 9 hours ago, 12 flags -
Watching TV
Jokes, Puns, & Pranks: 1 hours ago, 1 flags
active topics
-
Qatar kicks out HAMAS
Middle East Issues • 20 • : bastion -
RFK is Trumps health pick
2024 Elections • 4 • : soulrevival -
President-Elect DONALD TRUMP's 2nd-Term Administration Takes Shape.
Political Ideology • 192 • : MetalThunder -
Alex Jones Reinstated on X
Education and Media • 87 • : MetalThunder -
The art of being offended
Social Issues and Civil Unrest • 35 • : Flyingclaydisk -
Watching TV
Jokes, Puns, & Pranks • 1 • : PorkChop96 -
President-elect TRUMP Picks MATT GAETZ for his ATTORNEY GENERAL - High Level PANIC Ensues.
2024 Elections • 74 • : SideEyeEverything1 -
US warship Edsall Lost after Pearl Harbor Attack Found 80 Years Later ... by Accident
Mainstream News • 15 • : 38181 -
Mike Tyson returns 11-15-24
World Sports • 32 • : Encia22 -
Thanksgiving 2024
Member Art • 17 • : Flyingclaydisk