It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

Israeli deaths after the 1st jab being covered up? 40x Deaths than from Covid
page: 2share:
originally posted by: Rob808
Something about 78% covid hospitalizations in America were also obese?
originally posted by: dug88
a reply to: 111DPKING111
Seems pretty logical. On one hand, you've got a virus that over a year has been shown to be, overwhelmingly, only primarily deadly to the extreme elderly or health compromised individual...not many others...on the other hand you've got an experimental treatment with barely any testing created by companies with extremely shady histories that are totally exempt globally from liability over damages.
Which do you think is likely to cause more longterm harm and damage?
Wasn't there an article a while back that said diabetes, kidney problems and hypertension where the main risk factors, all of which have connections to being over weight?
originally posted by: Brotherman
originally posted by: dragonridr
a reply to: Brotherman
Yes if someone in a nursing home gets Covid they should be either quarantined or removed immediately.
In Pennsylvania if you have COVID they put you in the nursing home unit for COVID to keep the other hospitals operational. Around here they put residents in a different wing and consolidated them and clear floors for the 5 people that show up with the sniffles. Older folks in my neck of the woods are not happy.
Since most if not all tested for Covid are false positives this policy will obviously spread the disease further. Another big blunder for big dumb government. Is there any smart people left on the planet????
Man!!!!!!!!!!!!!!! Hitler would be loving the world today. And they even had their own politicians release the eugenics vaccine on them. All the Jew haters should be thrilled but they are never happy.
edit on 16-3-2021 by Doctor Smith because: added more brilliant thoughts
originally posted by: chr0naut
a reply to: 111DPKING111
Number of COVID-19 vaccine doses administered worldwide as of March 14, 2021, by country - Statista
Seems like more than 9 million in Israel. Israel is also using the Pfizer/Biontech vaccine.
The US government is tracking any issues with vaccines. As the USA has more doses of COVID-19 vaccines delivered than any other country, its data is likely to be the most representative of any issues: Vaccine Adverse Event Reporting System (VAERS) Data - HHS.govt
VAERS is good but it is not the end all be all, it is based on voluntary reports. If some entity or company doesn't report an "adverse event" it's not in here as well as reports aren't verified. Below is data DIRECT from VAERS today. Totals could be less or a lot more.
Considering the political and financial implications it's likely more. I'm in no way saying people should or shouldn't take the vaccine, but tell people 1174 people may have died from the vaccine and then let them choose.
I'd ask Marvin and Hank if they would take the vaccine again? oops, you can't cause they are dead after taking the vaccine.
Both Aaron and Hagler were in relatively good health for their age. This needs to be discussed and the media is leaving out details either on purpose or from governmental pressure.
SEE TODAYS CHART BELOW.
1174 DEATHS 805 CASES of full-blown COVID
VAERS accepts reports of adverse events and reactions that occur following vaccination. Healthcare providers, vaccine manufacturers, and the public can submit reports to VAERS. While very important in monitoring vaccine safety, VAERS reports alone cannot be used to determine if a vaccine caused or contributed to an adverse event or illness. The reports may contain information that is incomplete, inaccurate, coincidental, or unverifiable. Most reports to VAERS are voluntary, which means they are subject to biases. This creates specific limitations on how the data can be used scientifically. Data from VAERS reports should always be interpreted with these limitations in mind.
The strengths of VAERS are that it is national in scope and can quickly provide an early warning of a safety problem with a vaccine. As part of CDC and FDA's multi-system approach to post-licensure vaccine safety monitoring, VAERS is designed to rapidly detect unusual or unexpected patterns of adverse events, also known as "safety signals." If a safety signal is found in VAERS, further studies can be done in safety systems such as the CDC's Vaccine Safety Datalink (VSD) or the Clinical Immunization Safety Assessment (CISA) project. These systems do not have the same limitations as VAERS, and can better assess health risks and possible connections between adverse events and a vaccine.
Key considerations and limitations of VAERS data:
Vaccine providers are encouraged to report any clinically significant health problem following vaccination to VAERS, whether or not they believe the vaccine was the cause.
Reports may include incomplete, inaccurate, coincidental and unverified information.
The number of reports alone cannot be interpreted or used to reach conclusions about the existence, severity, frequency, or rates of problems associated with vaccines.
VAERS data are limited to vaccine adverse event reports received between 1990 and the most recent date for which data are available.
VAERS data do not represent all known safety information for a vaccine and should be interpreted in the context of other scientific information.

originally posted by: putnam6
originally posted by: chr0naut
a reply to: 111DPKING111
Number of COVID-19 vaccine doses administered worldwide as of March 14, 2021, by country - Statista
Seems like more than 9 million in Israel. Israel is also using the Pfizer/Biontech vaccine.
The US government is tracking any issues with vaccines. As the USA has more doses of COVID-19 vaccines delivered than any other country, its data is likely to be the most representative of any issues: Vaccine Adverse Event Reporting System (VAERS) Data - HHS.govt
VAERS is good but it is not the end all be all, it is based on voluntary reports. If some entity or company doesn't report an "adverse event" it's not in here as well as reports aren't verified. Below is data DIRECT from VAERS today. Totals could be less or a lot more.
Considering the political and financial implications it's likely more. I'm in no way saying people should or shouldn't take the vaccine, but tell people 1174 people may have died from the vaccine and then let them choose.
I'd ask Marvin and Hank if they would take the vaccine again? oops, you can't cause they are dead after taking the vaccine.
Both Aaron and Hagler were in relatively good health for their age. This needs to be discussed and the media is leaving out details either on purpose or from governmental pressure.
SEE TODAYS CHART BELOW.
1174 DEATHS 805 CASES of full-blown COVID
VAERS accepts reports of adverse events and reactions that occur following vaccination. Healthcare providers, vaccine manufacturers, and the public can submit reports to VAERS. While very important in monitoring vaccine safety, VAERS reports alone cannot be used to determine if a vaccine caused or contributed to an adverse event or illness. The reports may contain information that is incomplete, inaccurate, coincidental, or unverifiable. Most reports to VAERS are voluntary, which means they are subject to biases. This creates specific limitations on how the data can be used scientifically. Data from VAERS reports should always be interpreted with these limitations in mind.
The strengths of VAERS are that it is national in scope and can quickly provide an early warning of a safety problem with a vaccine. As part of CDC and FDA's multi-system approach to post-licensure vaccine safety monitoring, VAERS is designed to rapidly detect unusual or unexpected patterns of adverse events, also known as "safety signals." If a safety signal is found in VAERS, further studies can be done in safety systems such as the CDC's Vaccine Safety Datalink (VSD) or the Clinical Immunization Safety Assessment (CISA) project. These systems do not have the same limitations as VAERS, and can better assess health risks and possible connections between adverse events and a vaccine.
Key considerations and limitations of VAERS data:
Vaccine providers are encouraged to report any clinically significant health problem following vaccination to VAERS, whether or not they believe the vaccine was the cause.
Reports may include incomplete, inaccurate, coincidental and unverified information.
The number of reports alone cannot be interpreted or used to reach conclusions about the existence, severity, frequency, or rates of problems associated with vaccines.
VAERS data are limited to vaccine adverse event reports received between 1990 and the most recent date for which data are available.
VAERS data do not represent all known safety information for a vaccine and should be interpreted in the context of other scientific information.
VAERS may not be perfect, but the thing is, is there a better source of data on adverse reactions to vaccines?
Since at this point in the USA, more than 28 million doses of the COVID-19 vaccines have been given, and we have no way of knowing if those few deaths are actually because of the vaccine, or simply happened at the same time.
One thing we might look at is the normal average death rate in the USA in 1219 year (prior to the vaccine) per day, per 1000 population. The number is 8.782 deaths per thousand people, per day.
U.S. Death Rate 1950-2021
So, multiply that by 14 million (assuming 2 doses per person, so we divide the number of doses in half) /1000 (the previous figure was per 1000), and we get 122,000 deaths per day in a population of 14 million.
If we assume that most COVID-19 vaccinations have really only happened in the last month, then we must multiply 122,000 deaths by 30 days (approx.) which equals 3,660,000 deaths in the same period.
Next, we need to weed out the deaths of types that could not possibly be caused by a vaccine (shootings, car accidents, etc). Perhaps we should only include deaths by cytokine storm or blood clot only? We can look up death by cause tables for that. Of course the mortality tables don't divide up like that but we can use some common sense and eliminate most causes of death, leaving those from Influenza, Stroke and Respiratory diseases, which total to 356,767 out of a total of 2,854,838 (*note how far below the 3,660,000 figure the total deaths for 2019 are) which is 12.497% of total deaths.
Leading Causes of Death Data for the U.S.
So, 12.497% of 3,660,000 is 457,390 deaths that should normally be expected in this population size.
Now compare that to the 1,174 deaths in VARS. It would seem that the deaths which may possibly be caused by the COVID-19 vaccine/s are only 0.257% of of those that would be expected to occur normally in that number of people, in that period, and from those causes.
So either the stats are lies, and even have been falsified before COVID-19 existed, or, the vaccines are all proving to be extremely safe.
edit on 16/3/2021 by chr0naut because: (no reason given)
excessive deaths after vaccination?
now you finally know where deagel got its world wide population reduction numbers from
now you finally know where deagel got its world wide population reduction numbers from
I know a guy who took the two jabber.
Second jab put him in bed and out of working order for a week!
Second jab put him in bed and out of working order for a week!
a reply to: Homefree
This is information people need to be told as well when taking. The first shot is 85% effective and most of the negative reactions are from the 2nd, is 2nd jab worth it?
www.forbes.com...
The VAERS numbers should be told, along with the fact that a third of the deaths happen within 24 hours. Reddit has enough users you can get a decent feel for whats going on if you know where to look.
www.reddit.com...
People are speculating this Israeli death spike is due to a compromised immunity the week after the first shot, maybe taking ivermectin would be a safety precaution worth doing. Of course it would be nice if they acknowledged it and investigated to know for sure..
This is information people need to be told as well when taking. The first shot is 85% effective and most of the negative reactions are from the 2nd, is 2nd jab worth it?
www.forbes.com...
The VAERS numbers should be told, along with the fact that a third of the deaths happen within 24 hours. Reddit has enough users you can get a decent feel for whats going on if you know where to look.
www.reddit.com...
People are speculating this Israeli death spike is due to a compromised immunity the week after the first shot, maybe taking ivermectin would be a safety precaution worth doing. Of course it would be nice if they acknowledged it and investigated to know for sure..
edit on 17-3-2021 by 111DPKING111 because: (no reason given)
Why are they using the VAERS database to analyse Israeli deaths? # data in = # data out.
VAERS is US data. The US has a population over roughly 40x Israel so including that data is obviously going to provide a false positive reading 40x greater than the actual reading.
VAERS is US data. The US has a population over roughly 40x Israel so including that data is obviously going to provide a false positive reading 40x greater than the actual reading.
only 1 out of 4 congress people have got the shot. Just thought I would throw that out there.
Turns out the 'engineers' research was a post on a webforum, not a paper or statistical analysis. He works for 'GreenMedInfo'' selling quack remedies
and has no medical or mathematical knowlege - www.nakim.org...
They're an anti-vax group who make ridiculous claims like 'no one died from illness before vaccines were invented', 'wireless internet causes ADHD' and long disproven claim vaccines cause autism. childrenshealthdefense.org...
It had basic errors in the model like using US VAERS death data and comparing it to Ynet claims of the Israeli death total. No adjustments were made despite the US population being 40x Israels.
It falsely infered people are immune the second they recieve the first dose.
It falsely assumed 100% of deaths were due to the vaccine with no adjustment for naturally high death rate in the elderly.
There were also basic mathematical errors as there were only two deaths in people under 60. It also took most of it's data from facebook posts and false data published by Ynet rather than medical/statistical sources.
There was deliberate lying with numbers as the only stat he didn't publish from the table would have proven a reduction.
The figures using proper mathematics and scientific method show vaccnination groups rate is 0.2% that of unvacinated groups.
Tl;dr - engineers are crap at maths and logic, journalists are even worse but worst of all are quacks who lie about qualifications and public health data to sell nonsense remedies to gullible people.
They're an anti-vax group who make ridiculous claims like 'no one died from illness before vaccines were invented', 'wireless internet causes ADHD' and long disproven claim vaccines cause autism. childrenshealthdefense.org...
It had basic errors in the model like using US VAERS death data and comparing it to Ynet claims of the Israeli death total. No adjustments were made despite the US population being 40x Israels.
It falsely infered people are immune the second they recieve the first dose.
It falsely assumed 100% of deaths were due to the vaccine with no adjustment for naturally high death rate in the elderly.
There were also basic mathematical errors as there were only two deaths in people under 60. It also took most of it's data from facebook posts and false data published by Ynet rather than medical/statistical sources.
There was deliberate lying with numbers as the only stat he didn't publish from the table would have proven a reduction.
The figures using proper mathematics and scientific method show vaccnination groups rate is 0.2% that of unvacinated groups.
Tl;dr - engineers are crap at maths and logic, journalists are even worse but worst of all are quacks who lie about qualifications and public health data to sell nonsense remedies to gullible people.
edit on 17-3-2021 by bastion because: (no reason given)
edit on 17-3-2021 by
bastion because: (no reason given)
originally posted by: bastion
Why are they using the VAERS database to analyse Israeli deaths? # data in = # data out.
VAERS is US data. The US has a population over roughly 40x Israel so including that data is obviously going to provide a false positive reading 40x greater than the actual reading.
Perhaps because it is highly validated data on the effectiveness and adverse reactions to vaccines. And the Pfizer/BioNTech COVID-19 vaccine used almost exclusively in Israel, is also one used in the US, in large numbers of doses, and research like this data is shared between countries for their individual national approval authorities.
originally posted by: 111DPKING111
a reply to: Homefree
This is information people need to be told as well when taking. The first shot is 85% effective and most of the negative reactions are from the 2nd, is 2nd jab worth it?
www.forbes.com...
The VAERS numbers should be told, along with the fact that a third of the deaths happen within 24 hours. Reddit has enough users you can get a decent feel for whats going on if you know where to look.
www.reddit.com...
People are speculating this Israeli death spike is due to a compromised immunity the week after the first shot, maybe taking ivermectin would be a safety precaution worth doing. Of course it would be nice if they acknowledged it and investigated to know for sure..
The vaccines reaches maximum response 28 days after the first injection (as does just about any other vaccine, because immune response takes time and is dependent more on our biology that upon the specific formulation).
The Pfizer/BioNTech vaccine is procedurally delivered in two doses, the second being given close to 14 days (but less than 21 days) after the first. Maximum effectiveness is reached about 28 days afterwards, this even applied before it was found that a second dose was required to maximize the permanence of immune response.
edit on 18/3/2021 by chr0naut because: (no reason given)
F A K E
Imagine being dumb enough to fall for this more-than-obvious scam
Innocuous means: innocuous
Imagine being dumb enough to fall for this more-than-obvious scam
Innocuous means: innocuous
a reply to: chr0naut
They're probably the best source in the world on such data but the guy has used it in a deliberately misleading way to support his claims of an 'NWO vaccine holocaust'. I wasn't doubting VAERS, just rang alarm bells straight away as it introduces mass error and assumption for no reason and there's no reason for an Israeli computing student to understand the US VAERS data or how it is collated.
He uses monthly total deaths of a any cause as recorded in VAERS and compares these to daily total US Covid deaths. He also claims an incorrect figure of 3000 deaths for that period when the actual figure was 196 (including suicides, cancer. murder etc..)
He then acts suprised when his results don't match those of qualified mathematicians and medical journals and claims this is due to a global NWO euthanasia super conspiracy instead of the 100s of flaws in his methodology.
It's a fantastic example of how not to conduct a statistical analysis or what the public should look out for in bad science and why not to believe stats claims - it has a couple of percentage sums and graphs to give the impression it's sciency but there's no scienific or mathematical method used in his forum posts.
They're probably the best source in the world on such data but the guy has used it in a deliberately misleading way to support his claims of an 'NWO vaccine holocaust'. I wasn't doubting VAERS, just rang alarm bells straight away as it introduces mass error and assumption for no reason and there's no reason for an Israeli computing student to understand the US VAERS data or how it is collated.
He uses monthly total deaths of a any cause as recorded in VAERS and compares these to daily total US Covid deaths. He also claims an incorrect figure of 3000 deaths for that period when the actual figure was 196 (including suicides, cancer. murder etc..)
He then acts suprised when his results don't match those of qualified mathematicians and medical journals and claims this is due to a global NWO euthanasia super conspiracy instead of the 100s of flaws in his methodology.
It's a fantastic example of how not to conduct a statistical analysis or what the public should look out for in bad science and why not to believe stats claims - it has a couple of percentage sums and graphs to give the impression it's sciency but there's no scienific or mathematical method used in his forum posts.
originally posted by: bastion
a reply to: chr0naut
They're probably the best source in the world on such data but the guy has used it in a deliberately misleading way to support his claims of an 'NWO vaccine holocaust'. I wasn't doubting VAERS, just rang alarm bells straight away as it introduces mass error and assumption for no reason and there's no reason for an Israeli computing student to understand the US VAERS data or how it is collated.
He uses monthly total deaths of a any cause as recorded in VAERS and compares these to daily total US Covid deaths. He also claims an incorrect figure of 3000 deaths for that period when the actual figure was 196 (including suicides, cancer. murder etc..)
He then acts suprised when his results don't match those of qualified mathematicians and medical journals and claims this is due to a global NWO euthanasia super conspiracy instead of the 100s of flaws in his methodology.
It's a fantastic example of how not to conduct a statistical analysis or what the public should look out for in bad science and why not to believe stats claims - it has a couple of percentage sums and graphs to give the impression it's sciency but there's no scienific or mathematical method used in his forum posts.
Cheers for 'deep diving' into the provenance, and details of the data.
Unfortunately, there will be some issues related to the vaccine, that was expected, but the vaccine so far is proving to be extremely safe. Probably more so than any previous vaccine.
I would guess that the advantage of an mRNA vaccine compared with a 'killed' whole virus vaccine, means that there are fewer 'sideline factors' being targeted into immune response, and so the vaccine is safer overall.
edit on 18/3/2021 by chr0naut because: (no reason given)
a reply to: chr0naut
No worries, it was a good excuse to use applied maths to kill lockdown boredom.
Personally I think vaccinating people in 'end of life' or palative care makes no sense as there was no testing on frail elderly people. The data indicates ~90% of VAERS death from any cause are women over 85 - this may be due to elevated death risk in this age group, the vaccine itself or the way it is administered causing people stress or exposing them to more risk of getting Coronavirus than they would experience in the care home (personally I think the latter).
I think anyone who decides to take the vaccine should double check with their doctors and any specialists thet see, especially if they have any health conditions or are on medication. In the UK specialists ruling out any all interactions before it is available to people with those conditions - I don't think other countries are doing that or ruling out all possibilty the person may have Coronavirus before giving the injection.
It's annecdotal but every pregnant or breastfeeding woman I know had been advised by their GP not to have the vaccine. It's been deemed safe by OBGYN and MRHA plus mRNA should be far safer as it can't enter the womb or affect a developing foetus. The UK GOV advise is always check with Dr or specialist before getting the vaccine.
It appears the US, EU, Israel aren't being as cautious but the UK MRHA is one of the strictest in the world and only granted vaccine manufacturers a temporary licence, banned them from marketing and imposed strict conditions on the manufacturers that if broken result in an automatic ban from selling this and any other medicines in the UK. By law all vaccine centres must have epi pens to deal with any anaphalactic shock.
When I had mine nurses and Drs chose the AZ vaccine as I had a very bad allergic reaction to epillepsy medication last year and the AZ vaccine had been recommended by neuro, gp, epi nurse and consultant as their data shows it is the safest on the market
We have a Yellow Card system that acts like VAERS here: Yellow Card
The review of AstraZenica is here - AZ Side effects - PDF format buy from .gov site
It's far more detailed than VAERS as its aimed at medical profesionals and gives a breakdown of every reaction type and adverse event 28 days after vaccination.
AZ is causing fewer side-efects like sore arm and rapid heartbeat or blood clotting in the UK - other countries have suspended it over blood clot fears the cause could be political or differences in how the vaccine is administered. At the moment there simply isn't the data.
No worries, it was a good excuse to use applied maths to kill lockdown boredom.
Personally I think vaccinating people in 'end of life' or palative care makes no sense as there was no testing on frail elderly people. The data indicates ~90% of VAERS death from any cause are women over 85 - this may be due to elevated death risk in this age group, the vaccine itself or the way it is administered causing people stress or exposing them to more risk of getting Coronavirus than they would experience in the care home (personally I think the latter).
I think anyone who decides to take the vaccine should double check with their doctors and any specialists thet see, especially if they have any health conditions or are on medication. In the UK specialists ruling out any all interactions before it is available to people with those conditions - I don't think other countries are doing that or ruling out all possibilty the person may have Coronavirus before giving the injection.
It's annecdotal but every pregnant or breastfeeding woman I know had been advised by their GP not to have the vaccine. It's been deemed safe by OBGYN and MRHA plus mRNA should be far safer as it can't enter the womb or affect a developing foetus. The UK GOV advise is always check with Dr or specialist before getting the vaccine.
It appears the US, EU, Israel aren't being as cautious but the UK MRHA is one of the strictest in the world and only granted vaccine manufacturers a temporary licence, banned them from marketing and imposed strict conditions on the manufacturers that if broken result in an automatic ban from selling this and any other medicines in the UK. By law all vaccine centres must have epi pens to deal with any anaphalactic shock.
When I had mine nurses and Drs chose the AZ vaccine as I had a very bad allergic reaction to epillepsy medication last year and the AZ vaccine had been recommended by neuro, gp, epi nurse and consultant as their data shows it is the safest on the market
We have a Yellow Card system that acts like VAERS here: Yellow Card
The review of AstraZenica is here - AZ Side effects - PDF format buy from .gov site
It's far more detailed than VAERS as its aimed at medical profesionals and gives a breakdown of every reaction type and adverse event 28 days after vaccination.
AZ is causing fewer side-efects like sore arm and rapid heartbeat or blood clotting in the UK - other countries have suspended it over blood clot fears the cause could be political or differences in how the vaccine is administered. At the moment there simply isn't the data.
originally posted by: bastion
a reply to: chr0naut
No worries, it was a good excuse to use applied maths to kill lockdown boredom.
Personally I think vaccinating people in 'end of life' or palative care makes no sense as there was no testing on frail elderly people. The data indicates ~90% of VAERS death from any cause are women over 85 - this may be due to elevated death risk in this age group, the vaccine itself or the way it is administered causing people stress or exposing them to more risk of getting Coronavirus than they would experience in the care home (personally I think the latter).
I think anyone who decides to take the vaccine should double check with their doctors and any specialists thet see, especially if they have any health conditions or are on medication. In the UK specialists ruling out any all interactions before it is available to people with those conditions - I don't think other countries are doing that or ruling out all possibilty the person may have Coronavirus before giving the injection.
It's annecdotal but every pregnant or breastfeeding woman I know had been advised by their GP not to have the vaccine. It's been deemed safe by OBGYN and MRHA plus mRNA should be far safer as it can't enter the womb or affect a developing foetus. The UK GOV advise is always check with Dr or specialist before getting the vaccine.
It appears the US, EU, Israel aren't being as cautious but the UK MRHA is one of the strictest in the world and only granted vaccine manufacturers a temporary licence, banned them from marketing and imposed strict conditions on the manufacturers that if broken result in an automatic ban from selling this and any other medicines in the UK. By law all vaccine centres must have epi pens to deal with any anaphalactic shock.
When I had mine nurses and Drs chose the AZ vaccine as I had a very bad allergic reaction to epillepsy medication last year and the AZ vaccine had been recommended by neuro, gp, epi nurse and consultant as their data shows it is the safest on the market
We have a Yellow Card system that acts like VAERS here: Yellow Card
The review of AstraZenica is here - AZ Side effects - PDF format buy from .gov site
It's far more detailed than VAERS as its aimed at medical profesionals and gives a breakdown of every reaction type and adverse event 28 days after vaccination.
AZ is causing fewer side-efects like sore arm and rapid heartbeat or blood clotting in the UK - other countries have suspended it over blood clot fears the cause could be political or differences in how the vaccine is administered. At the moment there simply isn't the data.
What you propose is entirely reasonable.
Because I live in New Zealand, and we have the epidemic entirely controlled, we have no real urgency to roll out the vaccine.
Although the vaccine is being given to frontline staff in NZ, that may be exposed to the virus, I have not seen any public roll-out evidence at this stage. The government has undertaken to immunize all NZ'ers who want the vaccine within the next year.
The NZ government has decided the Pfizer/BioNTech vaccine should (at this stage) be the one chosen for all New Zealanders. This clears up any potential confusion about 'who gets what' vaccine and simplifies the dispensation procedurally (I think that Pfizer vaccine also has the highest published effectiveness rating).
The NZ government has pre-purchased sufficient vaccine to immunize the entire population of the country, but it is not mandatory, so any unused stocks will be donated to other Pacific nations around us, to create a 'safety bubble' in the region.
Also in the latest news, the EMA (European Medicines Agency) has ruled that the Oxford-AstraZeneca vaccine is "not associated" with a higher risk of blood clots, and is "safe and effective", and all the EU countries that had put the vaccine on hold, have now resumed their roll-outs.
edit on 19/3/2021 by chr0naut because: (no reason given)
a reply to: bastion
They have been asking the health ministry for additional information about who was vaccinated vs who died.
They are claiming morality 40x higher than other years and have written responses to several fact checkers.
www.nakim.org...
One possibility
"It should not be unexpected that Covid-19 vaccines have deleterious as well as intended effects. Pfizer data shows significant lymphocyte depletion in the first week after vaccination"
If you decide to vaccinate, maybe take Ivermectin or some other anti-viral before the jab.
"As reported by former New York Times journalist Alex Berenson, while Covid-19 mortality escalated among Israelis throughout January, in Palestine it declined steeply after a surge in December. Yet the Palestinians had no vaccine"
Its interesting the blood clots are getting attention for a few cases vs this situation
They have been asking the health ministry for additional information about who was vaccinated vs who died.
They are claiming morality 40x higher than other years and have written responses to several fact checkers.
www.nakim.org...
One possibility
"It should not be unexpected that Covid-19 vaccines have deleterious as well as intended effects. Pfizer data shows significant lymphocyte depletion in the first week after vaccination"
If you decide to vaccinate, maybe take Ivermectin or some other anti-viral before the jab.
"As reported by former New York Times journalist Alex Berenson, while Covid-19 mortality escalated among Israelis throughout January, in Palestine it declined steeply after a surge in December. Yet the Palestinians had no vaccine"
Its interesting the blood clots are getting attention for a few cases vs this situation
edit on 20-3-2021 by 111DPKING111 because: (no reason
given)
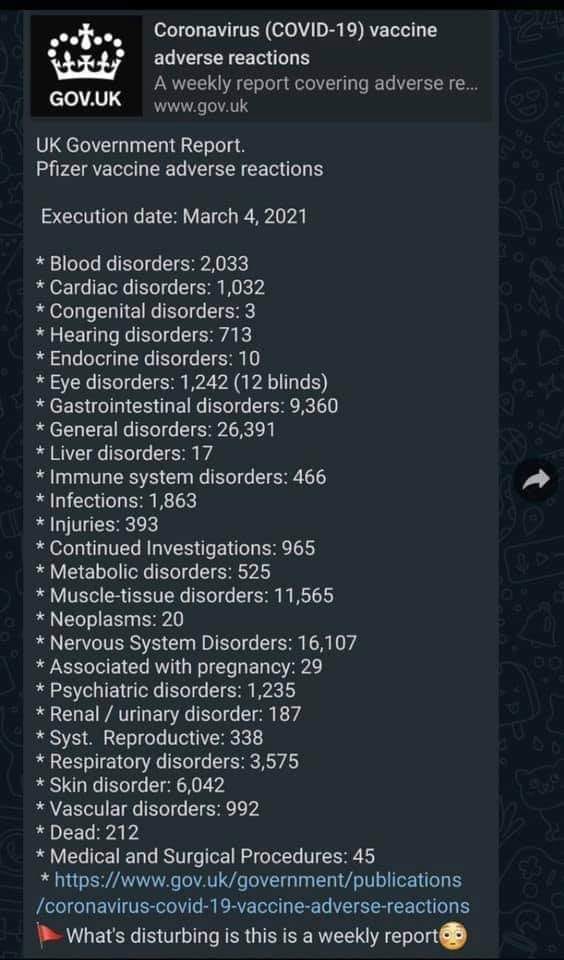
a reply to: angelchemuel
It's an edited one pushed on facebook - .gov yellow card doesn't use emojis in their data. They've almost doubled the stats and falsely claim it's from one week instead of cumulative total since vaccination began on 9th Dec. All this is clearly stated on the .gov and yellow card site.
This is the problem with people who don't understand data twisting it to fit their narative and pushing it to the public in viral social media posts.
These are reported events that occur within 28 days of vaccination - they're not proven to be caused by the vaccine. Over 10m people have had the Pfizer vaccine with 35,325 yellow cards.
.G OV Yellow Card data
As it's only the elderly and people with serious health conditions who recieve the vaccine in the UK it's obvious there will be a lot of health events that occur in that period. The yellow card system clearly states this and that they're not proof the vaccine was the cause of the health event.
Nearly all side effects are sore arm, bit of a headache and nausea and chills that pass in a couple of days. The real world data in the UK matches the safety profile and results of the clinical trials with no cause for alarm so far.
For example the morning after vaccination my eyes had a strange mild tight/pressure feeling - it wasn't painful or uncomfy and cleared up after a couple of hours but it was a strange feeling I've never had before which I'm pretty certain was due to the vaccine and is nearly all the eye disorders reported via yellow card.
a reply to: 111DPKING111
With the Palestine situation, he's not taken into account that Palestine was put under strict total lockdown in Dec and Jan and people could only leave their house to go to hospital after dark or at weekends. All movement was banned between Gaza, Israel and West bank.
Every country that has implemented lockdown has seen cases take a sharp decrease around a month after introduction, these are far stricter measures than used in the West so a more significant decrease is expected.
It's not logical and breaks the scientific method to claim a decrease in a country that doesn't have a vaccine (due to Israel having promised to supply Palestian vaccines but is still refusing to give it to non-Jewish settlers) means events in another country under a completely different economy, culture, healhcare system must be due to a vaccine or any other object.
By the same logic one could claim because less people die of cancer in the Vatican from Cancer than in the US, raping young boys or eating comunion wafers is the cure for cancer - correlation doesn't imply causation. Real world differences and world events need to be accounted for in any modelling to create an accurate model.
He doesn't use any of the mathematics that would allow him to do this, only a statistical engineer would be aware of the applied mathematics required to make such a model. A real model is full of multi-variable calculus, ordinary differential equations, applied Laplace equation, vectors, second order differential equations, lineaer combinations of random variables and loads of other boring stuff used in the creation stastical modeling and probability.
It's an edited one pushed on facebook - .gov yellow card doesn't use emojis in their data. They've almost doubled the stats and falsely claim it's from one week instead of cumulative total since vaccination began on 9th Dec. All this is clearly stated on the .gov and yellow card site.
This is the problem with people who don't understand data twisting it to fit their narative and pushing it to the public in viral social media posts.
These are reported events that occur within 28 days of vaccination - they're not proven to be caused by the vaccine. Over 10m people have had the Pfizer vaccine with 35,325 yellow cards.
Up to and including 7 March 2021, the MHRA received and analysed 35,325 UK Yellow Cards from people who have received the COVID-19 mRNA Pfizer/BioNTech vaccine. These reports include a total of 100,810 suspected reactions (i.e. a single report may contain more than one symptom). The first report was received on 9 December 2020.
.G OV Yellow Card data
As it's only the elderly and people with serious health conditions who recieve the vaccine in the UK it's obvious there will be a lot of health events that occur in that period. The yellow card system clearly states this and that they're not proof the vaccine was the cause of the health event.
Nearly all side effects are sore arm, bit of a headache and nausea and chills that pass in a couple of days. The real world data in the UK matches the safety profile and results of the clinical trials with no cause for alarm so far.
For example the morning after vaccination my eyes had a strange mild tight/pressure feeling - it wasn't painful or uncomfy and cleared up after a couple of hours but it was a strange feeling I've never had before which I'm pretty certain was due to the vaccine and is nearly all the eye disorders reported via yellow card.
edit on 20-3-2021 by bastion because: (no reason given)
a reply to: 111DPKING111
With the Palestine situation, he's not taken into account that Palestine was put under strict total lockdown in Dec and Jan and people could only leave their house to go to hospital after dark or at weekends. All movement was banned between Gaza, Israel and West bank.
Every country that has implemented lockdown has seen cases take a sharp decrease around a month after introduction, these are far stricter measures than used in the West so a more significant decrease is expected.
It's not logical and breaks the scientific method to claim a decrease in a country that doesn't have a vaccine (due to Israel having promised to supply Palestian vaccines but is still refusing to give it to non-Jewish settlers) means events in another country under a completely different economy, culture, healhcare system must be due to a vaccine or any other object.
By the same logic one could claim because less people die of cancer in the Vatican from Cancer than in the US, raping young boys or eating comunion wafers is the cure for cancer - correlation doesn't imply causation. Real world differences and world events need to be accounted for in any modelling to create an accurate model.
He doesn't use any of the mathematics that would allow him to do this, only a statistical engineer would be aware of the applied mathematics required to make such a model. A real model is full of multi-variable calculus, ordinary differential equations, applied Laplace equation, vectors, second order differential equations, lineaer combinations of random variables and loads of other boring stuff used in the creation stastical modeling and probability.
edit on 20-3-2021 by bastion because: (no reason given)
new topics
-
Thanksgiving 2024
Member Art: 3 hours ago -
The art of being offended
Social Issues and Civil Unrest: 5 hours ago -
FLORIDA Sues Biden-Harris FEMA for Denying Disaster Assistance to Homeowners with TRUMP Signs.
US Political Madness: 6 hours ago -
Turns out, they planned to go after P-nut.
US Political Madness: 10 hours ago
top topics
-
Turns out, they planned to go after P-nut.
US Political Madness: 10 hours ago, 20 flags -
The art of being offended
Social Issues and Civil Unrest: 5 hours ago, 15 flags -
FLORIDA Sues Biden-Harris FEMA for Denying Disaster Assistance to Homeowners with TRUMP Signs.
US Political Madness: 6 hours ago, 12 flags -
Sick sick sick ---graphic story
Social Issues and Civil Unrest: 16 hours ago, 7 flags -
Thanksgiving 2024
Member Art: 3 hours ago, 5 flags
active topics
-
Encouraging News Media to be MAGA-PAF Should Be a Top Priority for Trump Admin 2025-2029.
Education and Media • 68 • : WeMustCare -
Thanksgiving 2024
Member Art • 6 • : CarlLaFong -
President-elect TRUMP Picks MATT GAETZ for his ATTORNEY GENERAL - High Level PANIC Ensues.
2024 Elections • 57 • : marg6043 -
The Trump effect 6 days after 2024 election
2024 Elections • 113 • : cherokeetroy -
WATCH LIVE: US Congress hearing on UFOs, unidentified anomalous phenomena
Aliens and UFOs • 52 • : putnam6 -
FLORIDA Sues Biden-Harris FEMA for Denying Disaster Assistance to Homeowners with TRUMP Signs.
US Political Madness • 29 • : Dandandat3 -
The Acronym Game .. Pt.4
General Chit Chat • 952 • : JJproductions -
HHS Spent Hundreds of Millions of Dollars on DEI Initiatives Under Biden, Watchdog Finds
US Political Madness • 7 • : VariedcodeSole -
The art of being offended
Social Issues and Civil Unrest • 21 • : Kaiju666 -
Should we look for the truth, or just let it go?
US Political Madness • 120 • : chr0naut