It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

What makes COVID-19 worse than Seasona Influenza in one pic
page: 3share:
originally posted by: Aallanon
a reply to: Edumakated
Who’s numbers are you going to trust? Chinese? Italy’s? Saudi Arabia?
I don’t even trust the numbers I’m getting from the USA
I don't know...
But what I do know is the stock market tanked, schools shut down, business shut down, people out of work, and I can't find a decent roll of double ply toilet paper; yet all we can report is 100 or so deaths tied to this virus right now. 6000 cases.
Tragic? Yes? Worthy of losing out collective sh*t over? Not in the slightest. Particularly, when we know for fact tens of thousand die every year already from the flu and tens of million get infected.
With the data they keep telling us about infection rate and severity, I'd expect to see people dying in the streets by now. Yet, it hasn't happened and don't give me the bull about it just started and incubation periods.
originally posted by: Krakatoa
Here's a great source of actual data, assessment,s and projections based upon the UK models that would also apply to the USA (only delayed by a few weeks).
16-MAR- 2020: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand
Reposting again here for those that missed it and are asking for the data.
a reply to: Edumakated
Why? Too many movies perhaps?
I'd expect to see people dying in the streets by now.
originally posted by: Aallanon
a reply to: Edumakated
Who’s numbers are you going to trust? Chinese? Italy’s? Saudi Arabia?
I don’t even trust the numbers I’m getting from the USA
you shouldnt trust US numbers. While South Korea tested over 290 thousand people, US tested 38 thousand.
If somebody dies with symptoms but without getting tested, they are not added to the casualties. This explain why the death rate in US is low compared to other countries
originally posted by: Phage
a reply to: Krakatoa
That's a 20 page pdf.
You don't expect anyone to read that, do you?
20 pages!
It has the answers....if they REALLY want them.
I went through it, took me about 30 minutes to digest and then the light went on. This is a source that has NO politics involved. I trust it more than anything I've read to date.
originally posted by: Krakatoa
originally posted by: Phage
a reply to: Krakatoa
That's a 20 page pdf.
You don't expect anyone to read that, do you?
20 pages!
It has the answers....if they REALLY want them.
I went through it, took me about 30 minutes to digest and then the light went on. This is a source that has NO politics involved. I trust it more than anything I've read to date.
Post a few of the important snippets from it?
originally posted by: Phage
a reply to: Edumakated
Why? Too many movies perhaps?
I'd expect to see people dying in the streets by now.
No, because that is what we are being told is / was going to happen. All the info / data / govt response is saying post apocalyptic prepper wet dream, yet here we are....
You are a smart guy... yet, some how you can't seem to notice none of the stuff is adding up?
a reply to: Edumakated
By a few on ATS (and the like), perhaps. Other than that, not so much.
No, because that is what we are being told is / was going to happen.
edit on 3/18/2020 by Phage because: (no reason given)
originally posted by: FredT
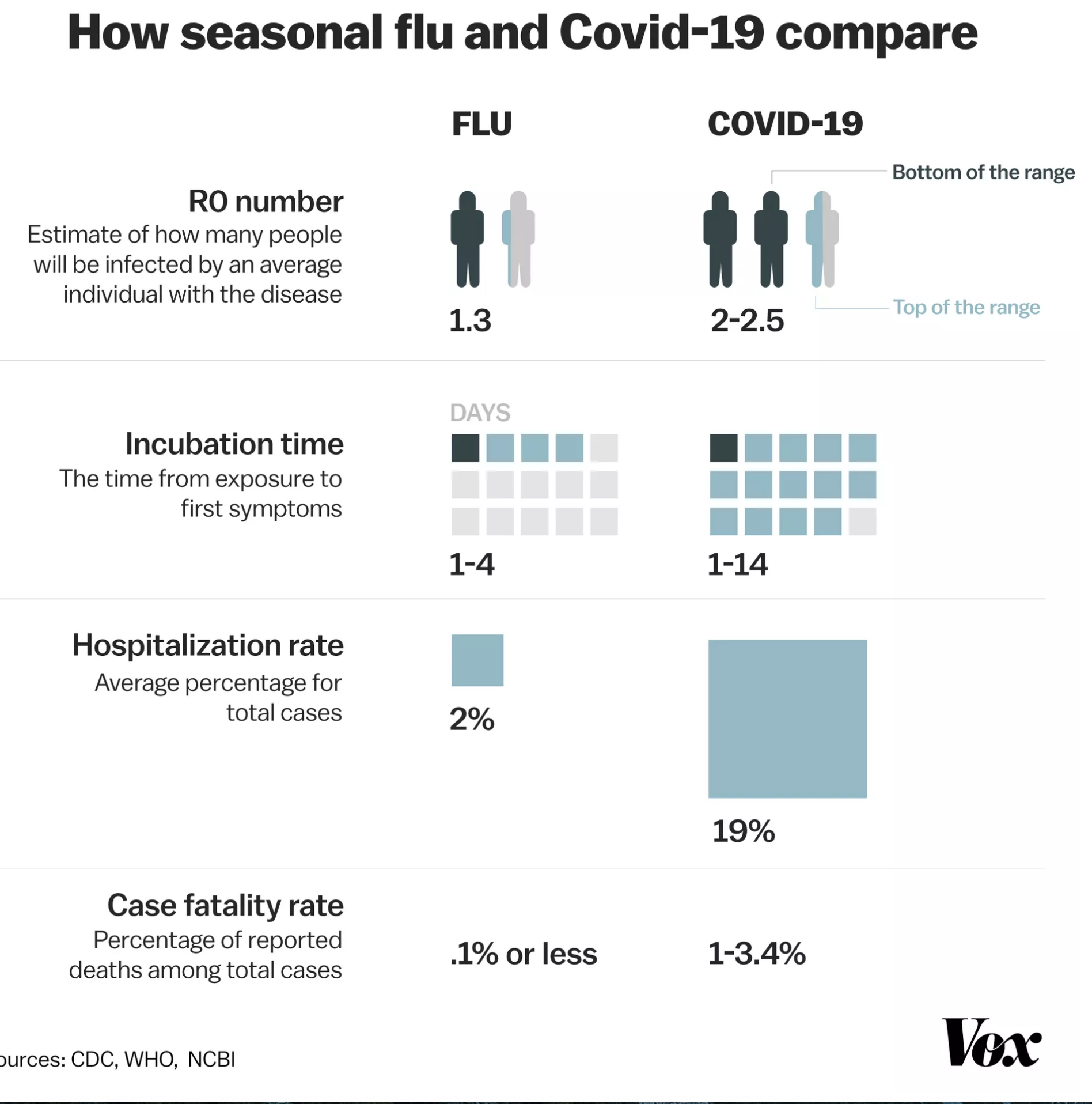
While at this point the total numbers make seasonal influenza more deadly that's not bearing per infection. This chart by the CDC and WHO really sums things up. The incubation period, the spread and need to hospitalize are simply way way greater and at some point the number of case will jump as we start ramping up testing. This is why we need to flatten the curve to allow the healthcare system to deal with it.
www.vox.com...
Even so, considering that at this point in time this is the best and most honest info we have on this virus, the question nobody asks is this:
Does this data justify the extreme measures taken who will have catastrophic consequences economically, financially, socially and politically all around the world?
edit on 18-3-2020 by WhiteHat because: (no reason given)
originally posted by: carewemust
a reply to: nugget1
If you go to Italy and ask around, I bet almost everyone knows someone who knows someone who knows someone who is in the hospital, or has died from the virus.
In America you would have to ask a whole lot of people before finding someone who knows someone who knows someone who is hospitalized, or who has died from Coronavirus.
You're quite right.
The uptick in numbers of elderly dying at home is probably coincidental. Same with rising numbers of deaths in nursing homes. No autopsies, and even if there were they're not testing for covid.
Even if Covid was going through the nursing homes, the 4 ICU beds our hospital has wouldn't be much good.
Plausible deniability makes the most sense. The masses have already gone into a frenzied panic- our Walmart is completely out of canned goods.
*sigh*
edit on 300000044America/Chicago311 by nugget1 because: eta
a reply to: Krakatoa
I'm not saying it's you because I don't know if you have or not, but I'm tired of people pushing this fear that Coronavirus is so much more deadly than the flu, so much more contagious, and hangs around for so much longer, yet never answer the hard questions that would undermine that argument
Since the OP never got back to me, maybe you can answer these questions everyone that's pushing the Coronavirus scare.
How did they determine the Coronavirus has a 19% hospitalization rate?
How do they calculate the percentage of people dying from Coronavirus if they don't know how many people have actually had the Coronavirus?
If the Coronavirus is so much more contagious, then why are there only 217K cases compared to 29 million flu cases?
Would it be a safe assumption to say that 10's of millions of people have had the Coronavirus, but they've only detected 217k because those are the people that got checked out?
If there are indeed 10's of millions of cases that have gone undetected, wouldn't that decrease the mortality rate dramatically?
I'm not saying it's you because I don't know if you have or not, but I'm tired of people pushing this fear that Coronavirus is so much more deadly than the flu, so much more contagious, and hangs around for so much longer, yet never answer the hard questions that would undermine that argument
Since the OP never got back to me, maybe you can answer these questions everyone that's pushing the Coronavirus scare.
How did they determine the Coronavirus has a 19% hospitalization rate?
How do they calculate the percentage of people dying from Coronavirus if they don't know how many people have actually had the Coronavirus?
If the Coronavirus is so much more contagious, then why are there only 217K cases compared to 29 million flu cases?
Would it be a safe assumption to say that 10's of millions of people have had the Coronavirus, but they've only detected 217k because those are the people that got checked out?
If there are indeed 10's of millions of cases that have gone undetected, wouldn't that decrease the mortality rate dramatically?
At this point it no longer matters. I do believe Covid is more contagious than Influenza but only time will tell if it is more deadly. Doesn't matter
tho because the world's economies are ravaged.
Even if you never get Covid-19, or never know a single person who dies from it, you will most certainly know many people who will suffer economically for a long time after this is over.
Even if you never get Covid-19, or never know a single person who dies from it, you will most certainly know many people who will suffer economically for a long time after this is over.
originally posted by: Krakatoa
Here's a great source of actual data, assessment,s and projections based upon the UK models that would also apply to the USA (only delayed by a few weeks).
16-MAR- 2020: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand
Since some can't be bothered with actual reading or doing the research to answer their questions, Here are some highlights from the above source. If you want a more granular answer, I highly recommend to spend the time to actually read it for yourself.
Two fundamental strategies are possible: (a) mitigation, which focuses on slowing but not necessarily
stopping epidemic spread – reducing peak healthcare demand while protecting those most at risk of
severe disease from infection, and (b) suppression, which aims to reverse epidemic growth, reducing
case numbers to low levels and maintaining that situation indefinitely. Each policy has major
challenges. We find that that optimal mitigation policies (combining home isolation of suspect cases,
home quarantine of those living in the same household as suspect cases, and social distancing of the
elderly and others at most risk of severe disease) might reduce peak healthcare demand by 2/3 and
deaths by half. However, the resulting mitigated epidemic would still likely result in hundreds of
thousands of deaths and health systems (most notably intensive care units) being overwhelmed many
times over. For countries able to achieve it, this leaves suppression as the preferred policy option.
The major challenge of suppression is that this type of intensive intervention package –
or something equivalently effective at reducing transmission – will need to be maintained until a
vaccine becomes available (potentially 18 months or more) – given that we predict that transmission
will quickly rebound if interventions are relaxed.
Epidemic timings are approximate given the limitations of
surveillance data in both countries: The epidemic is predicted to be broader in the US than in GB and
to peak slightly later. This is due to the larger geographic scale of the US, resulting in more distinct
localised epidemics across states (Figure 1B) than seen across GB. The higher peak in mortality in GB is due to the smaller size of the country and its older population compared with the US. In total, in an
unmitigated epidemic, we would predict approximately 510,000 deaths in GB and 2.2 million in the
US, not accounting for the potential negative effects of health systems being overwhelmed on
mortality.
Our
projections show that to be able to reduce R to close to 1 or below, a combination of case isolation,
social distancing of the entire population and either household quarantine or school and university
closure are required (Figure 3, Table 4). Measures are assumed to be in place for a 5-month duration.
Not accounting for the potential adverse effect on ICU capacity due to absenteeism, school and
university closure is predicted to be more effective in achieving suppression household quarantine.
All four interventions combined are predicted to have the largest effect on transmission (Table 4).
Such an intensive policy is predicted to result in a reduction in critical care requirements from a peak
approximately 3 weeks after the interventions are introduced and a decline thereafter while the
intervention policies remain in place.
new topics
-
Nov 2024 - Former President Barack Hussein Obama Has Lost His Aura.
US Political Madness: 42 minutes ago -
Something better
Dissecting Disinformation: 5 hours ago -
The Witcher IV — Cinematic Reveal Trailer | The Game Awards 2024
Video Games: 8 hours ago -
Friday thoughts
General Chit Chat: 9 hours ago -
More Ons?
Political Conspiracies: 9 hours ago -
Canada Post strike ended by the Government of Canada
Mainstream News: 9 hours ago
top topics
-
They Know
Aliens and UFOs: 13 hours ago, 18 flags -
Something better
Dissecting Disinformation: 5 hours ago, 8 flags -
More Ons?
Political Conspiracies: 9 hours ago, 6 flags -
Friday thoughts
General Chit Chat: 9 hours ago, 5 flags -
Canada Post strike ended by the Government of Canada
Mainstream News: 9 hours ago, 4 flags -
The Witcher IV — Cinematic Reveal Trailer | The Game Awards 2024
Video Games: 8 hours ago, 2 flags -
Drones (QUESTION) TERMINATOR (QUESTION)
General Chit Chat: 15 hours ago, 1 flags -
Nov 2024 - Former President Barack Hussein Obama Has Lost His Aura.
US Political Madness: 42 minutes ago, 1 flags
active topics
-
They Know
Aliens and UFOs • 60 • : CarlLaFong -
More Ons?
Political Conspiracies • 18 • : rickymouse -
Something better
Dissecting Disinformation • 13 • : Astrocometus -
-@TH3WH17ERABB17- -Q- ---TIME TO SHOW THE WORLD--- -Part- --44--
Dissecting Disinformation • 3669 • : xuenchen -
Nov 2024 - Former President Barack Hussein Obama Has Lost His Aura.
US Political Madness • 1 • : xuenchen -
A Bunch of Maybe Drones Just Flew Across Hillsborough County
Aircraft Projects • 68 • : Zaphod58 -
DONALD J. TRUMP - TIME's Most Extraordinary Person of the Year 2024.
Mainstream News • 39 • : WeMustCare -
The Acronym Game .. Pt.4
General Chit Chat • 1012 • : FullHeathen -
USS Liberty - I had no idea. Candace Owen Interview
US Political Madness • 33 • : DEATHANDTRUTH -
And Here Come the Excuses!!
General Conspiracies • 201 • : cherokeetroy