It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

nCoV and Seizure - Crossing the Blood Brain Barrier
page: 1share:
Coronavirus has been reported to cause viral encephalitis in children, not nCov, but its older cousins. Keep in mind this is new research, I'm
learning just reading about it because it used to be significantly delayed damage. This means I was incorrect a week or so ago when I said it was
unlikely and would be delayed if it even happened.
Neurologic Alterations Due to Respiratory Virus Infections
Some of these symptoms could be present in those videos, because we're not immune, the symptoms could be worse and move faster. Anything from partial seizures to going into full status or a grand mal full body seizure.
There is more bad news, all of our airway membranes including the nasopharynx are loaded with ACE2 receptors, the primary binding site of nCoV. Watch how that works out with SARS-CoV, nCoV's closest relative in humans.
Sound familiar? Looks like a severe nCoV infection with complications that we are hearing about online, they will both present similarly in systemic patients. There is also the problem of how deep this infection can go because our body has ACE2 receptors everywhere.
Keep in mind, a systemic infection significantly increases the chance of cytokine storm or septic shock. Inflammation is supposed to be local, targeted only to infected tissue. You can see its impact in a hand if you cut yourself, it gets warm as vessels dilate, increasing blood flow, you feel heat as a result, sometimes there is pain. As the vessels dilate, they also increase in permeability so your white blood cells can move into infected tissue. If this happens in the entire body, you see a blood pressure drop, severe fever, leaky blood vessels and this can severely impact the lungs as the patient begins to crash.
Finally, lets look at some rodent studies using a very similar virus, mouse hepatitis virus and human corona-virus.
Demyelination is bad, myelin is an insulating sheath for your neurons to send electrical signals through nervous tissue and the body. Without it, those signals can become jumbled, problematic, influence signaling and even cause an electrical storm in your brain. Severe cases could result in a seizure.
You do not want to be in a pro-inflammatory state in the brain, this can increase the chance of seizures. Looking back at the table earlier, encephalitis can result in inflamed membranes which can initiate a seizure.
They do need more studies, test results and epidemiological studies confirm that CoVs can cross the blood brain barrier. They do want to perform more animal studies to demonstrate how this is possible. We could be seeing this happen in people at an increased rate because of the seemingly high morbidity rate of this virus. I do hope this isn't the case, you never know, its brand new.
Neurologic Alterations Due to Respiratory Virus Infections
Among these neuropathological viruses are the human respiratory syncytial virus (hRSV), the influenza virus (IV), the coronavirus (CoV) and the human metapneumovirus (hMPV) [...] The most frequent clinical manifestations described in these patients are febrile or afebrile seizures, status epilepticus, encephalopathies and encephalitis. All these viruses have been found in cerebrospinal fluid (CSF), which suggests that all these pathogens, once in the lungs, can spread throughout the body and eventually reach the CNS.

Some of these symptoms could be present in those videos, because we're not immune, the symptoms could be worse and move faster. Anything from partial seizures to going into full status or a grand mal full body seizure.
Remarkably, neurotropic and neuro-invasive capabilities have been described in several of their hosts, including humans among them, leading to symptoms such as multiple sclerosis (MS) and encephalomyelitis [...] However, the capacity of CoV to infect CNS in humans is not well characterized, with their detection in these samples performed mainly by detection of viral RNA, exhibiting persistent infection.
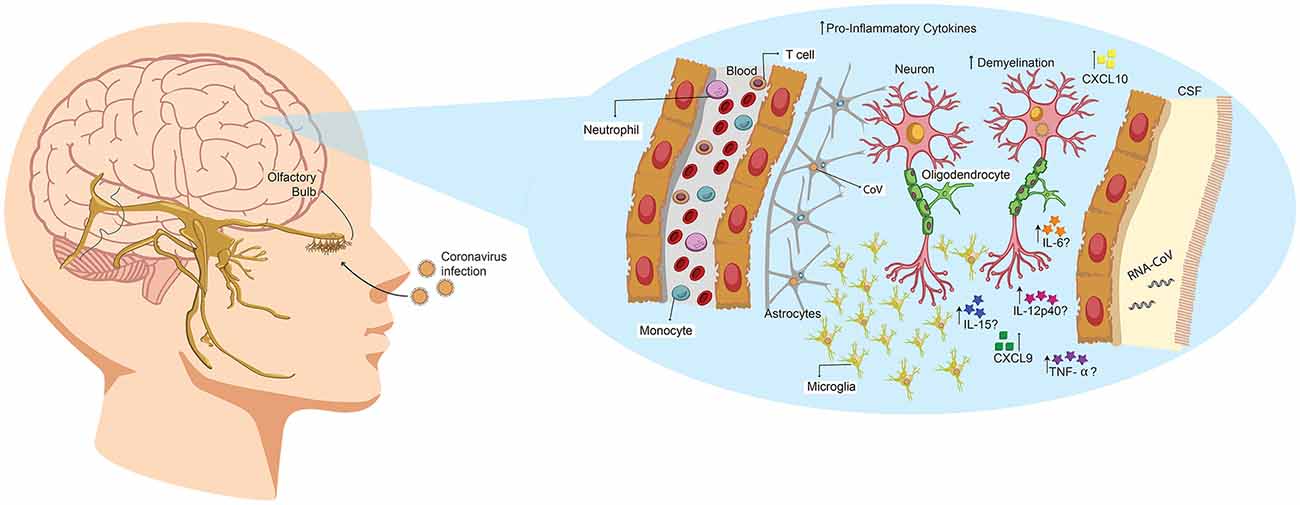
Figure 3. Human coronavirus (HCoV) enters the CNS through the olfactory bulb, causing inflammation and demyelination. Upon nasal infection, HCoV can reach the CNS through the olfactory bulb, as ablation of this part of the brain restricts its neurotropic capacities in mice. Once the infection is set, the virus can reach the whole brain and CSF in less than 7 days. Accordingly, it has been described that this virus can induce demyelination. Likewise, primary glial cultures have been described to secrete IL-6, IL-12p40, IL-15, TNF-α, CXCL9 and CXCL10 upon viral infection.
There is more bad news, all of our airway membranes including the nasopharynx are loaded with ACE2 receptors, the primary binding site of nCoV. Watch how that works out with SARS-CoV, nCoV's closest relative in humans.
The first case of SARS-CoV infection with neurological manifestations was reported the year 2003 in a 59-year-old woman. She was first admitted with swinging fever, chills, productive coughing and diarrhea, which eventually lead to oxygen requirements, vomit, seizures and episodes of four-limb twitching. The respiratory failure continued until she was sedated, and ventilation was required. SARS-CoV infection was confirmed in both tracheal aspirates and CSF samples, followed by ribavirin treatment, with no improvement in seizures persistence. With additional treatments, seizures were no longer detected, and she was discharged 3 weeks after admission.
Sound familiar? Looks like a severe nCoV infection with complications that we are hearing about online, they will both present similarly in systemic patients. There is also the problem of how deep this infection can go because our body has ACE2 receptors everywhere.
Organ dissemination of SARS-CoV in autopsy samples from patients that died of this disease was determined. The report indicates the presence of SARS-CoV-N protein and viral RNA in the stomach, small intestine, kidney, sweat glands, parathyroid, pituitary gland, liver and cerebrum, further confirming the capacity of this virus to induce a systemic infection.
Keep in mind, a systemic infection significantly increases the chance of cytokine storm or septic shock. Inflammation is supposed to be local, targeted only to infected tissue. You can see its impact in a hand if you cut yourself, it gets warm as vessels dilate, increasing blood flow, you feel heat as a result, sometimes there is pain. As the vessels dilate, they also increase in permeability so your white blood cells can move into infected tissue. If this happens in the entire body, you see a blood pressure drop, severe fever, leaky blood vessels and this can severely impact the lungs as the patient begins to crash.
Finally, lets look at some rodent studies using a very similar virus, mouse hepatitis virus and human corona-virus.
HCoV capacity to reach CNS after the nasal infection has been described previously in mice, particularly for HCoV-OC43. St-Jean et al. (2004) reported that upon infection, viral antigens are detected in the olfactory bulb 3 days later, with no presence of virus in perivascular blood cells or any other part of the brain. After 7 days, the virus is detected throughout the whole brain tissue, indicating that it can rapidly propagate once set in CNS. This replication leads to a rapid death by acute encephalitis of infected mice.
Mice studies are mainly performed with MHV, a virus that belongs to the BCoV genus and is genetically related to HCoV-OC43; likewise, the disease at CNS as elucidated by both viruses are similar, as they both induce demyelination [...] Jacomy and Talbot (2003) were among the first to describe a mouse model to characterize the CNS disease in their publication the year 2003. Therein, they exhibit that BALB/c and C57BL/6 mice could be infected through nasal instillation with MHV, although they chose to use intracerebral inoculation to favor CNS infection. They also determined that viral RNA could be detected in brain, heart, spleen, lungs, liver and muscles.
Demyelination is bad, myelin is an insulating sheath for your neurons to send electrical signals through nervous tissue and the body. Without it, those signals can become jumbled, problematic, influence signaling and even cause an electrical storm in your brain. Severe cases could result in a seizure.
Finally, in Jacomy et al. (2006) described that HCoV-OC43 could infect glial and neuronal cells of both rat and mice (Figure 3). Therein, they also showed that surviving animals exhibited decreased motor functions. [...] According to this, glial primary cultures of MHV-A59-infected cells showed an increase in the secretion of IL-12 p40, TNF-α, IL-15 and IL-6 compared with a non-neurotropic MHV, suggesting that the infection with a neurotropic virus activates glial cells and induces a pro-inflammatory state.
You do not want to be in a pro-inflammatory state in the brain, this can increase the chance of seizures. Looking back at the table earlier, encephalitis can result in inflamed membranes which can initiate a seizure.
CoVs are respiratory viruses that exhibit neurotropic capacities that not only allows them to achieve latency and avoid the immune response of the host, but also have neurological implications that can complicate the disease associated to its infection.
They do need more studies, test results and epidemiological studies confirm that CoVs can cross the blood brain barrier. They do want to perform more animal studies to demonstrate how this is possible. We could be seeing this happen in people at an increased rate because of the seemingly high morbidity rate of this virus. I do hope this isn't the case, you never know, its brand new.
I think some common viruses can do this to some extent too. Febrile seizures seem common these days from viruses. My grandkids had some febrile
seizures when they were sick, which is common. The hospital said that the virus was not influenza, but it was a virus of some kind for sure. Now,
maybe some viruses can do this as part of their ability to cause seizures. Chemicals from microbes can get through the BB barrier, and some small
microbes without an outer shell can too.
a reply to: rickymouse
Seizures are scary, in most cases they look way worse than they actually are. It all depends on the underlying pathology. My son has them, ranging from micro to partial to going into status.
What worries me about this research is inflammatory signaling can increase chances of that crossover. We’re also not immune to this thing yet and we are at a major disadvantage at fighting during the initial period.
I’m also concerned that this virus has a long incubation period and there is evidence of CoV using a latent period to hide from the immune system. What if it only infects the upper airway in some patients, symptoms go away and it moves through the olfactory into the brain. A few days later, they have headaches and odd neurological symptoms, then they suddenly go down because it either stays in the brain or becomes systemic.
It’s interesting, I would gladly take viral pneumonia over viral encephalitis with possible neurological complications. I love watching and researching how it moves but it’s terrible at the same time.
Seizures are scary, in most cases they look way worse than they actually are. It all depends on the underlying pathology. My son has them, ranging from micro to partial to going into status.
What worries me about this research is inflammatory signaling can increase chances of that crossover. We’re also not immune to this thing yet and we are at a major disadvantage at fighting during the initial period.
I’m also concerned that this virus has a long incubation period and there is evidence of CoV using a latent period to hide from the immune system. What if it only infects the upper airway in some patients, symptoms go away and it moves through the olfactory into the brain. A few days later, they have headaches and odd neurological symptoms, then they suddenly go down because it either stays in the brain or becomes systemic.
It’s interesting, I would gladly take viral pneumonia over viral encephalitis with possible neurological complications. I love watching and researching how it moves but it’s terrible at the same time.
a reply to: TheAMEDDDoc
So if the novel coronavirus doesn’t present symptoms in some people and the blood/brain barrier is broken, we could be seeing some of the infected keeling over and going into a seizure many weeks after infection?
So if the novel coronavirus doesn’t present symptoms in some people and the blood/brain barrier is broken, we could be seeing some of the infected keeling over and going into a seizure many weeks after infection?
a reply to: butcherguy
Theoretically yes, it’s happened in animal models. Or they could just have mild symptoms and it goes away and they get the encephalitis symptoms.
We have no concrete data, it’s spreading through so much of their population, it’s bound to happen. It happened with SARS and that was a much smaller group.
It can also happen in pretty much any patient on any end of the spectrum. It does happen with other diseases too, including seasonal ones but we are usually partially immune to those diseases in most cases.
Theoretically yes, it’s happened in animal models. Or they could just have mild symptoms and it goes away and they get the encephalitis symptoms.
We have no concrete data, it’s spreading through so much of their population, it’s bound to happen. It happened with SARS and that was a much smaller group.
It can also happen in pretty much any patient on any end of the spectrum. It does happen with other diseases too, including seasonal ones but we are usually partially immune to those diseases in most cases.
originally posted by: butcherguy
a reply to: TheAMEDDDoc
So if the novel coronavirus doesn’t present symptoms in some people and the blood/brain barrier is broken, we could be seeing some of the infected keeling over and going into a seizure many weeks after infection?
Saw this the other day, so it's happening.
a reply to: Tekner
It could be, that’s a tough angle to make a judgement, it helps to see their eyes and face.
What stinks is we need test results either from an autopsy or through testing CSF to see if there are white blood cells or viral RNA in the brain, CSF or other organs.
With the current “burn everything” policy and their treatment protocols, we won’t know until a western facility gets a patient like this.
It could be, that’s a tough angle to make a judgement, it helps to see their eyes and face.
What stinks is we need test results either from an autopsy or through testing CSF to see if there are white blood cells or viral RNA in the brain, CSF or other organs.
With the current “burn everything” policy and their treatment protocols, we won’t know until a western facility gets a patient like this.
edit on 4-2-2020 by TheAMEDDDoc because: (no reason given)
I saw someone calling this seizure decorticate posturing on another thread.
Now that I have checked into it, it looks more like decerebrate posturing that I have seen in most of the twitter videos that I have watched that purport to show victims of the corona virus.
Now that I have checked into it, it looks more like decerebrate posturing that I have seen in most of the twitter videos that I have watched that purport to show victims of the corona virus.
a reply to: butcherguy
Maybe at the end but that’s quite some arm extension at the beginning with the limbs angled that way, really hard to tell with the blanket.
Checking eyes and face with vitals would confirm what happened followed by some imaging and diagnostic testing.
The movements are odd, epileptic seizures are more regular, sometimes focal or post secondary can get weird though. I need more info, don’t like his final resting position but they do weird stuff like that when they relax sometimes. Its almost looks like a seizure you would see in a TV show or movie.
It acts like a complete deregulation of signaling like you would see with exposure or inflammation like NMDA encephalitis, I’m just guessing and rambling. Only thing that looks like decorticate is at the end and it’s hard to see.
Maybe at the end but that’s quite some arm extension at the beginning with the limbs angled that way, really hard to tell with the blanket.
Checking eyes and face with vitals would confirm what happened followed by some imaging and diagnostic testing.
The movements are odd, epileptic seizures are more regular, sometimes focal or post secondary can get weird though. I need more info, don’t like his final resting position but they do weird stuff like that when they relax sometimes. Its almost looks like a seizure you would see in a TV show or movie.
It acts like a complete deregulation of signaling like you would see with exposure or inflammation like NMDA encephalitis, I’m just guessing and rambling. Only thing that looks like decorticate is at the end and it’s hard to see.
edit on 5-2-2020 by TheAMEDDDoc because: (no reason given)
originally posted by: butcherguy
I saw someone calling this seizure decorticate posturing on another thread.
Now that I have checked into it, it looks more like decerebrate posturing that I have seen in most of the twitter videos that I have watched that purport to show victims of the corona virus.
It was my thread. Can you please provide the example of the patient having decerebrate posturing?
a reply to: Violater1
I just watched that, I could see an aura, seizure and post-ictal state really well. Without more data it does not rule out encephalitis or another issue anywhere in the central nervous system. If I had to guess, that looked epileptic, just a little short for a coma like torpor state at the end, unless his tongue fell back into his airway and he went out.
They need to start ruling crap out instead of ruling one thing in and sending the body to the fires. We need to see how this thing moves in the body.
I just watched that, I could see an aura, seizure and post-ictal state really well. Without more data it does not rule out encephalitis or another issue anywhere in the central nervous system. If I had to guess, that looked epileptic, just a little short for a coma like torpor state at the end, unless his tongue fell back into his airway and he went out.
They need to start ruling crap out instead of ruling one thing in and sending the body to the fires. We need to see how this thing moves in the body.
originally posted by: TheAMEDDDoc
a reply to: Violater1
I just watched that, I could see an aura, seizure and post-ictal state really well. Without more data it does not rule out encephalitis or another issue anywhere in the central nervous system. If I had to guess, that looked epileptic, just a little short for a coma like torpor state at the end, unless his tongue fell back into his airway and he went out.
They need to start ruling crap out instead of ruling one thing in and sending the body to the fires. We need to see how this thing moves in the body.
YOU COULD SEE THE AURA!
REALLY?
REALLY!
ONLY THE PERSON HAVING THE SEIZURE CAN SEE THE AURA!
[snipped]
WE'RE THROUGH![snipped]
edit on Wed Mar 11 2020 by DontTreadOnMe because: (no reason given)
a reply to: Violater1
Some people can give physical cues to an aura, he grabbed his head and acted dizzy. My son will blink quickly, have mouth movement, and will sometimes get hyper. Not all auras are visible which is true. Some people get a weird taste or feeling etc. You said you were a medical professional?
Some people can give physical cues to an aura, he grabbed his head and acted dizzy. My son will blink quickly, have mouth movement, and will sometimes get hyper. Not all auras are visible which is true. Some people get a weird taste or feeling etc. You said you were a medical professional?
originally posted by: Violater1
originally posted by: butcherguy
I saw someone calling this seizure decorticate posturing on another thread.
Now that I have checked into it, it looks more like decerebrate posturing that I have seen in most of the twitter videos that I have watched that purport to show victims of the corona virus.
It was my thread. Can you please provide the example of the patient having decerebrate posturing?
I don't have the time to dig them up right now, but the ones that was referring to showed patients with their arms straightened out (slight bend in the elbows) in front of them, at about shoulder or face level. Their legs were straightened out and were shaking rapidly.
I thought that decorticate posturing involved the hands pulling in tight to the chest?
I am not a doctor.... I didn't even stay at the Holiday Inn.
Decorticate posture is an abnormal posturing in which a person is stiff with bent arms, clenched fists, and legs held out straight. The arms are bent in toward the body and the wrists and fingers are bent and held on the chest.
PennState Hershey Medical Center
edit on
b000000292020-02-07T15:24:15-06:0003America/ChicagoFri, 07 Feb 2020 15:24:15 -0600300000020 by butcherguy because: (no reason given)
a reply to: butcherguy
The seizures and collapsing do worry me overseas, but not many of the videos are showing either of these abnormal rigidity positions. You should definitely see them after the seizure if there is inflammation, pressure, demyelination or damage from neurotoxicity. You could also see the positioning at the beginning.
The problem is they’re not even really considering a treatment protocol for these issues. We’ve seen respiratory infections can cause inflammation and demyelination. If these patients are having these problems in the brain or spinal cord they need to test for that and treat it. For all we know, this virus could cross the blood brain barrier easier than others. Once that happens the patient will slowly suffer damage with each seizure and inflammatory event. Inflammation damages the protective coating and cuts off signaling and you could see seizures or abnormal rigidity.
Another issue is glutamate neurotoxicity which will destroy or cause scar tissue/sclerosis in the long term, increasing the chance of consecutive seizures and making them resistant to seizure medication and benzo intervention. If the patient has encephalitis or frequent seizures from this disease, they will need constant benzo management, seizure medications (Keppra, Vimpat, Depakene/Depakote) and steroids until the infection subsides. They are also usually placed in medically induced comas to prevent further damage. They keep them on an EEG and EKG monitor to watch for abnormal brain waves that look similar to epileptic activity. Then they are weaned off meds and released. In an epidemic like this, I see no way to really manage these patients.
Even these patients will experience the 3 stages of seizure. Aura is the first and can last hours, minutes or seconds. Patient will experience feelings, hallucinations, nausea, dizziness, altered mental status etc. These CAN be visualized by outside people, it’s why seizure dogs work. Seizure is the second stage, depending on length and underlying pathology, it can be a life threat and 5+ minutes, 15 if you’re an EMT is what is called going into status, patient cannot get oxygen and intervention is required. Post-ictal is the end state, abnormal posturing, torpor, sleep are very common and you can see jerky movements in many patients as the abnormal signaling begins to subside.
We saw it with SARS and MERS, we see it with other seasonal diseases so we will see it with nCoV. Without treatment it could cause death or permanent damage aand they need to test for viral RNA and white blood cells in CSF.
The seizures and collapsing do worry me overseas, but not many of the videos are showing either of these abnormal rigidity positions. You should definitely see them after the seizure if there is inflammation, pressure, demyelination or damage from neurotoxicity. You could also see the positioning at the beginning.
The problem is they’re not even really considering a treatment protocol for these issues. We’ve seen respiratory infections can cause inflammation and demyelination. If these patients are having these problems in the brain or spinal cord they need to test for that and treat it. For all we know, this virus could cross the blood brain barrier easier than others. Once that happens the patient will slowly suffer damage with each seizure and inflammatory event. Inflammation damages the protective coating and cuts off signaling and you could see seizures or abnormal rigidity.
Another issue is glutamate neurotoxicity which will destroy or cause scar tissue/sclerosis in the long term, increasing the chance of consecutive seizures and making them resistant to seizure medication and benzo intervention. If the patient has encephalitis or frequent seizures from this disease, they will need constant benzo management, seizure medications (Keppra, Vimpat, Depakene/Depakote) and steroids until the infection subsides. They are also usually placed in medically induced comas to prevent further damage. They keep them on an EEG and EKG monitor to watch for abnormal brain waves that look similar to epileptic activity. Then they are weaned off meds and released. In an epidemic like this, I see no way to really manage these patients.
Even these patients will experience the 3 stages of seizure. Aura is the first and can last hours, minutes or seconds. Patient will experience feelings, hallucinations, nausea, dizziness, altered mental status etc. These CAN be visualized by outside people, it’s why seizure dogs work. Seizure is the second stage, depending on length and underlying pathology, it can be a life threat and 5+ minutes, 15 if you’re an EMT is what is called going into status, patient cannot get oxygen and intervention is required. Post-ictal is the end state, abnormal posturing, torpor, sleep are very common and you can see jerky movements in many patients as the abnormal signaling begins to subside.
We saw it with SARS and MERS, we see it with other seasonal diseases so we will see it with nCoV. Without treatment it could cause death or permanent damage aand they need to test for viral RNA and white blood cells in CSF.
This corona-virus is sort of like Fips in cats, it creates a proteinase enzyme sort of like papain that destroys collagen and elastin and the blood
brain barrier is made primarily of collagen and elastin. Another proteinase can break down the CV proteinase. But if it is administered too late, it
cannot fix the damage in cats.
A naturally occurring proteinase found in pineapple stems and core can destroy that enzyme and also can destroy viruses to some extent, but if the disease has progressed to far already, adding another proteinase will further destroy the elastin and collagen. Prevention may be better than treatment, supplementing with bromelain may have beneficial effects before getting sick. Also monolaurin does soften and permeate the corona-virus's shell so our immune chemicals can destroy it. If you have enough stomach acid, lauric acid in coconut oil or even in butter will help protect you. It needs to be converted into monoglyceride of lauric acid to form bromelain, so since the bromelain temporarily destroys lypase too, you should take the coconut oil seperately from the proteinase. Bromelain is anti-inflammatory too, so it can help with swelling somewhat. Systematically it goes into the blood, so have it on an empty stomach for that, as a digestive aid, eat it with food and it will help our body break down proteins in the food.
Bromelain also denatures the Chondrosite enzyme that destroys lung tissue in COPD somewhat, I have more possible solutions to combating that too but no way of testing my theories because I do not have copd. I guess N-acetylsysteine does help to slow copd, after all it is the main ingredient in some of the copd meds. I am not sure if that supplement could help with the coronavirus at all.
Spell check does not help me much with the kind of words I am writing, so forgive the spelling errors.
A naturally occurring proteinase found in pineapple stems and core can destroy that enzyme and also can destroy viruses to some extent, but if the disease has progressed to far already, adding another proteinase will further destroy the elastin and collagen. Prevention may be better than treatment, supplementing with bromelain may have beneficial effects before getting sick. Also monolaurin does soften and permeate the corona-virus's shell so our immune chemicals can destroy it. If you have enough stomach acid, lauric acid in coconut oil or even in butter will help protect you. It needs to be converted into monoglyceride of lauric acid to form bromelain, so since the bromelain temporarily destroys lypase too, you should take the coconut oil seperately from the proteinase. Bromelain is anti-inflammatory too, so it can help with swelling somewhat. Systematically it goes into the blood, so have it on an empty stomach for that, as a digestive aid, eat it with food and it will help our body break down proteins in the food.
Bromelain also denatures the Chondrosite enzyme that destroys lung tissue in COPD somewhat, I have more possible solutions to combating that too but no way of testing my theories because I do not have copd. I guess N-acetylsysteine does help to slow copd, after all it is the main ingredient in some of the copd meds. I am not sure if that supplement could help with the coronavirus at all.
Spell check does not help me much with the kind of words I am writing, so forgive the spelling errors.
originally posted by: TheAMEDDDoc
...
Keep in mind, a systemic infection significantly increases the chance of cytokine storm or septic shock.
...
Interesting, thanks!
Could explain a few things - younger doctors dying (being constantly exposed, they may be more likely to develop a systemic infection), people dropping dead in the street, etc...
Will we ever really know the truth about this thing?
new topics
-
Azerbaijan E190 Passenger Jet Shot Down by Russia
Mainstream News: 4 hours ago -
Orange County Makes Shoplifting a Felony
Other Current Events: 8 hours ago -
It's Offical Now
US Political Madness: 10 hours ago -
The reason it works is.....
General Chit Chat: 11 hours ago
top topics
-
Orange County Makes Shoplifting a Felony
Other Current Events: 8 hours ago, 16 flags -
It's Offical Now
US Political Madness: 10 hours ago, 13 flags -
The reason it works is.....
General Chit Chat: 11 hours ago, 8 flags -
Dick Van Dyke saved from Wildfire by neighbours on his 99th birthday
People: 14 hours ago, 7 flags -
Azerbaijan E190 Passenger Jet Shot Down by Russia
Mainstream News: 4 hours ago, 5 flags
active topics
-
Azerbaijan E190 Passenger Jet Shot Down by Russia
Mainstream News • 10 • : yuppa -
Drones everywhere in New Jersey ---and Elsewhere Master Thread
Aliens and UFOs • 229 • : yuppa -
It's Offical Now
US Political Madness • 14 • : BernnieJGato -
DefCon Teetering on Escalation
World War Three • 49 • : ADVISOR -
London Christmas Market BANS Word ‘Christmas’
Social Issues and Civil Unrest • 45 • : Blaine91555 -
Orange County Makes Shoplifting a Felony
Other Current Events • 22 • : FeeshJefe -
Political Warfare & The Resister Special Forces Underground
Political Ideology • 1 • : ADVISOR -
The reason it works is.....
General Chit Chat • 4 • : randomuser2034 -
Dick Van Dyke saved from Wildfire by neighbours on his 99th birthday
People • 2 • : angelchemuel -
Post A Funny (T&C Friendly) Pic Part IV: The LOL awakens!
General Chit Chat • 7954 • : underpass61