It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

Carbs...Sugar...And Other Stuff
page: 1share:
Carbs, Sugar, and Other Stuff
This started out as a quick enquiry into the world of sugar, simple carbs, and Keto/low carb dieting. I was trying to figure out if what I do for my personal health was any better/worse than what others do, find out if sugar/simple carbs were the "devil", and see which diet, if any, I wanted to follow after researching the whole thing. It wasn't long before I had 30 pages of info to share.
I did what I normally do, took notes and wrote down thoughts about what I found. I tried to cover both sides of the story as best I could. But the journey was long and veered off into many different directions. Our food history is very complex and chaotic! There are so many different thoughts and opinions on what sugar/simple carbs do for/to you...I was a bit overwhelmed. But in the end, I found it was helpful. I gained some new perspectives and eating ideas. I realized a few things about my own eating habits, and I think I truly understand the whole "diet world" a bit better than what I did before.
I'm not going to share everything I found. The information went from sugar/simple carbs to advertising strategies to different types of body compositions...it would be just too much. I am going to share the basics. Which is still a huge amount of information. Nope, I'm not telling you how to live or what to eat, those are and have always been individual choices. What I'm trying to do is group all the information I've found in one spot making it easily accessible for myself and others.
I'm not making a statement or trying to prove something is good/bad for you. You can read and decide for yourself what you feel is relevant from the following pages. And this is not meant to demonize anything. It's just information. It's also a journey to finding the truth (my truth) and hopefully at the end of this thread, through unbiased reporting and listing everything I have uncovered, I'll have a clear view (and so will you) of how simple carbohydrates and refined sugars affect our lives.
I started from the beginning, the very beginning, and worked my forward into the modern day world. And, I use a lot of studies and other sources, so, you need to take into consideration some things as you are reading. Just as I had to take them into consideration while I was researching.
Things for consideration:
All data can be manipulated to achieve desired results. By the inclusion and exclusion of certain variables, the deductions or conclusions can vary as well. For example:
- Data may have different paths or conclusions using the same evidence.
- The amount of test subjects and the length of the study
- Who is doing the study (is it a research study provided by the company or an outside source?)
- The date of the study/article - is it old or new?
- The methodology used
These are just some examples of what you should be looking for when you read through this thread. There will be reference material at the end as well as links with each quote to the source. And, every source I quoted/used had multiple sources with the same ideas...none of it was just found in one place.
I didn't want this to be all one sided. It isn't fair to not present all the information I've collected. So, I've included an Opposing view for each major section. Whichever position you take with regards to the information, there are some valid points on each side to consider. I did my best to report what I found as fairly and accurately as possible. And, I tried to leave my own biases out of it all (I tried, don't know if I succeeded).
So, let's began....
edit on 4-2-2018 by blend57 because: Always an edit : /
Carbohydrate Origins
The introduction of carbohydrates into our diet happened in the Neolithic period. When we started to farm and produce simple grass grains such as maize, wheat, and corn. With that introduction came some noticeable and well documented physiological changes.
Paleontologists compared the remains of the hunter/gatherer man with the farming man and they showed some interesting results. One of the most prevalent differences was in the way our teeth developed. The hunter/gatherer had stronger, healthier teeth. There teeth were wider apart and more capable of chewing and breaking downs meats/proteins. With the introduction of agriculture, the spacing and make up of our teeth changed. They started to grow closer together which caused crooked, deformed teeth. The enamel became softer and wore through easier, tooth decay became an issue. It had not been an issue prior to the agriculture boom.
"It is accepted that masticatory forces regulate craniofacial growth and the stress is mainly due to the food consistency that causes variations in the mastication movement" (Sardi et al. 2004: 141). This means that facial structures are suited to individual chewing needs. When new preparation and processing methods were introduced, foods became softer and easier to chew. Over time this change in masticatory function contributed to an overall "gracilization" of the human skull and resulted in a smaller human face with reduced jaws and teeth (Larsen 1991, 2006; Sardi et al. 2004). Reduction of the face negatively affected human oral health because human teeth did not reduce proportionately to the jaw and crowding resulted (Larsen 2006). Dental crowding is problematic because it creates tight spaces between the teeth where bacteria can easily grow. These oral bacteria can contribute to plaque build-up and promotes caries, "an oral infectious disease [which] involves the demineralization of the enamel and the underlying dentin and other tissues, caused by the acids produced as a byproduct of the metabolism of dietary carbohydrates, especially sugars" (Larsen 2006:13). Increased occurrence of caries has generally been associated with agricultural lifestyles; however, a study in southeast Asia conducted by Tayes et al. (2000) found that caries decreased with the introduction of rice agriculture, suggesting that rice may be less cariogenic than other starchy staple foods which formed the subsistence base of other Neolithic cultures (Meller et al. 2009).
Similarly, Papathanasiou (2005) found that dental caries were present in low frequencies among the early agriculturalists of Alepotrypa Cave in Greece. Eshed et al. (2010:383) found a decrease in caries among the Neolithiceof the Levant. According to Meller et al. (2009:290), the maize-based diet associated with many prehistoric American agriculturalists was "rich in sticky carbohydrates and sucrose ... thereby, the physical and chemical properties of maize, probably combined with its preparation methods, seem to provide a 96 cariogenic potential in the oral environment." In the Americas there is a clear relationship between maize-based agriculture and increased occurrence of caries (Larsen 1991; Meller et al. 2009; Tayes et al. 2000). Microwear analysis suggests that the new food processing methods of the Neolithic combined with consumption of softer foods may have contributed to caries as well as attrition. "Microwear is displayed as pits and scratches on the teeth. The expression of these features is determined by the consistency of the foods consumed and/or the inclusion of extraneous particles introduced to the food when it is being prepared" (Larsen 2006:13). These "pits and scratches" create environments for cariogenic bacteria. When coarse foods are eaten regularly it wears down the microwear on teeth and helps prevent caries, but when softer foods are eaten the bacteria has an opportunity to thrive in these spaces (Meller et al. 2009). Residue from stones used to grind plant matter and, in dry environments, sand incorporated into foods, have been attributed to promoting caries as well as attrition in Neolithic populations in both the Old World as well as the Americas (Larson 2006; Meller et al. 2009; Papathanasiou 2005). While caries increased most markedly among the maize-based cultures of the Americas, populations of the Old World also saw a decline in oral health. Papathanasiou (2005) cited increases in premortem tooth loss and periodontal disease among the early Greek agriculturalists from Alepotrypa cave.
Periodontal disease, also known as gingivitis, can cause tooth loss and serious damage to the tissue and bone supporting the teeth (Larsen 2006; Papathanasiou 2005). Meller et al. (2009) reported similar findings among the Pica-Tarapaca culture of the Atacama Desert circa 1000 B.P. as well as among the Maya of Mexico. Eshed et al. (2010) cited a decrease in attrition and periodontal disease in the Levant but reported increased occurrence of calculus (tartar or plaque)
. ..
Quite a long quote, I know. But a more complete picture of what occurred during the Neolithic revolution regarding teeth than I could write myself. What it simply is saying is that we became more sedentary than hunter/gatherers, our jaw/facial bone structure changed, and that, coupled with our new eating habits created some serious dental issues.
But, it doesn't stop there. Our new carbohydrate diet changed a few other things as well. Iron deficiency and anemia were also more abundant within the Neolithic people. Shorter life spans (we are talking before the age of medicine) and height decreases have been directly linked to the new diet. There are other health issues that we developed during this time period such as new diseases, decline in fitness levels, and digestive issues. But, although they could be a direct result of our diet, I feel like they could also be a direct result of just settling down and enduring the climatic changes in one location. So, although the information is found in the links, I felt it should not be included as evidence when talking strictly about dietary changes.
Continued...

Opposing View
The opposing view asserts that even though there was a period of adjustment with our new diet, we eventually normalized again. As we made the dietary transition, our height and life spans returned to normal. Our tooth enamel began to stop de-mineralizing, thus decreasing the amount of cavities found in Neolithic humans to less than those found in hunter/gatherer humans. All the other issues that occurred with regards to our close proximity to animals, the new diseases, health issues, and overall decline in fitness levels normalized as well. This was about 2000 years ago. Basically what they are saying is we adapted. Which is what humans do.
Then a funny thing happened on the way from the preagricultural Mediterranean to the giant farms of today: people, at least some of them, got healthier, presumably as we adapted to the new way of life and food became more evenly distributed. The collection of skeletons from Egypt also shows that by 4,000 years ago, height had returned to its preagricultural levels, and only 20 percent of the population had telltale signs of poor nutrition in their teeth. Those trying to make the point that agriculture is bad for our bodies generally use skeletal material from immediately after the shift to farming as evidence, but a more long-term view is starting to tell a different story. For example, Timothy Gage of the State University of New York at Albany examined long-term mortality records from around the world, along with the likeliest causes of death, and concluded that life span did not decrease, nor did many diseases increase, after agriculture. Some illnesses doubtless grew worse after humans settled down, but life has had its “nasty, brutish, and short” phases at many points throughout history ...
An 18 page excerpt of the book Paleofantasy can be found here ...
Also, prior to the hunter/gatherer stage, humans were mostly foragers. Which means we relied on fruits, nuts, berries and vegetables in order to survive. I mention this just to make sure that all variables are present and presented. What this, in my mind, signifies is that we have cycled through a different type of diet at least once before and have managed to adapt to the new ways of eating eventually. I've not been able to find any real good articles/papers with regards to the initial change from foragers to meat eaters and how that affected our body as of yet.
The few existing dental remains reveal that the earliest hominids lived by gathering nuts, berries and other wild vegetation. Without tools, they were only able to consume meat by scavenging eggs or picking carcasses left by predators. Their body structure was that of an herbivore’s as well. A more prominent mandible with sizable grinding molars, such as those of Australopithecus anamensis, made it easier to break down plant fibers. A larger digestive tract with specialized enzymes aided their digestion. Yet, gradually, as primitive tool-making advanced, meat consumption rose dramatically ...
Through transitioning diets, we've had our bumps and bruises along the way. Brain growth/shrinkage, new diseases introduced and building immunities to them, etc...but we always seem to bounce back and adjust to the new diets/behaviors.
There is also new archeological evidence that places hominoids to much earlier time period than previously thought. What relevancy that has with regards to eating habits I'm unsure of. Would that change the date of the Neolithic Revolution or was there another dietary change in between the hunter/gather diet and agriculture boom. So far, I've not found any studies that show evidence of that happening. But as we learn more about our distant past, I'm sure we'll gather new insights into our diets as well.
Note: If transitioning to/from diets in the past showed evidence of deteriorating health and then a normalization of health, is that what we are going through today with the introduction of GMO's and lab/chemically altered foods? Will we see a decline and then normalization in health as we move forward and our bodies adapt to the newly introduced food sources?
Moving on....
edit on 4-2-2018 by blend57 because: (no reason given)

Sugar Origins
26% of all diabetes is caused by sugar in the united states. 25% worldwide.
There are 56 names for sugar
There are varying thoughts as to sugar's origins. The earliest reference I could find is that it was discovered in New Guinea in 8000 B.C. Around 6000 B.C. is was introduced to the Philippines and India, and there are mentions of it in Hindu religious documents dated 500 A.D. A written reference to sugar which is used is the reed which gives honey without bees . Which was said to be used to describe sugar cane by the Emperor Darious in 510 A.D. ...
The Egyptians had developed a rudimentary way to obtain sugar from honey in 1600 A.D. This is evidenced through hieroglyphs that notated the process which included fruits, nuts, herbs, and spices. ...
The recipe for tiger nut sweets was actually found on a broken piece of ancient Egyptian pottery and dated to around 1600 BCE, according to the American Research Center in Egypt. Although modern interpretations of the recipe use walnuts, almonds or both, the original recipe used tiger nuts, which are actually tubers of the Cyperus esculentus plant. The tiger nuts were chopped into small pieces and mixed with chopped dates, honey and spices, and then formed into small balls. Ancient Egyptians ate with their fingers, so these bite-sized balls may have been the perfect after-dinner treat or anytime snack.
The first chemically refined sugar was brought to us by India around 2500 years ago. But it was expensive, mainly a treat for only the wealthy to enjoy. Sugar became cheap/affordable in 1850, at which time we discovered how to extract it from sugar beets. It entered the US market in 1870. So, now we have two sources of sugar, sugar cane and sugar beets. Both are widely used today, along with corn sugar, which will be covered a little later on.
Again, I use the studies of curies in order to evaluate the affects sugar had on our bodies. There was a study done on the effects of sugar related caries around the world from the Neolithic period to modern times. You will find a ton of interesting information in it, well worth the read. But for the purpose of this thread, I'm only going to quote the conclusions. This is what they found based on the evidence extracted:
The available data indicates that the modern trends on caries increases start simultaneously with permanent growth intake of sucrose during the last two centuries. The hypotheses of an increase in the susceptibility or resistance diminishment by genetic reasons or the installation of a particularly cariogenic flora have not been sufficiently corroborated (De Soet & Laine, 2008; Hassell & Harris, 1995; Shuler, 2001; van Palenstein et al., 1996) while dietary changes seem to be the most reasonable answer. In the modern western world and increasingly in other regions of the globe approximately half of consumed calories comes from carbohydrates and almost half of it is sucrose.
Until recently, several populations living in isolated areas of the world kept their ancestral ways of life (for instance, many African tribes, Inuits, South American Indians, Melanesian, Polynesian) under conditions of perfect adaptation to their environments and diets (Donnelly et al., 1977; Mayhall, 1977; Pedersen, 1971; Schamschula et al., 1980; Walker & Hewlett, 1990). Bacteriologic analyses of their dental plaques, although not extensive, show cariogenic species, but those individuals are still developing few or no caries. Otherwise, when those populations were acculturated or simply replaced their traditional diet for an “occidental refined diet”, they started to develop progressively destructive caries patterns ...
The conclusions based on the evidence shows that not only did carbohydrates effect our dental health, but sugar did/does as well. The introduction of refined sugar seemed to have a direct impact, as by the last paragraph you can see that when isolated populations kept to their ancestral diet they showed less curies. When they switched over to the modern day diet, which is high in sugar and carbohydrates, their curies increased noticeably.
The end result of the study was that diet adaptations which included sucrose were a direct cause of the increase of curies within each country studied.
The available data indicates that the modern trends on caries increases start simultaneously with permanent growth intake of sucrose during the last two centuries. The hypotheses of an increase in the susceptibility or resistance diminishment by genetic reasons or the installation of a particularly cariogenic flora have not been sufficiently corroborated (De Soet & Laine, 2008; Hassell & Harris, 1995; Shuler, 2001; van Palenstein et al., 1996) while dietary changes seem to be the most reasonable answer. In the modern western world and increasingly in other regions of the globe approximately half of consumed calories comes from carbohydrates and almost half of it is sucrose.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)
The Opposing View
The same study shows that curies started to normalize again throughout the middle ages. Also, with the introduction of fluoride and dental care techniques, we are not seeing as many cavities as we once were. So, once again, you see a increase in dental issues and then a decrease as we adapt. Although, adaptation this time involves better oral care habits developed through gaining more knowledge of how curies and oral issues are caused. Basically, we have better science to help us through the transition stages of a refined sugar diet. And let's be honest, it is a diet that everyone adheres to because sugar and carbohydrates are in almost everything now a days.
Caries increase tendency seems to have been constant during the second half of the 19th century and the first half of the 20th century, worldwide. On the other hand, preventive policies against caries did not have considerable effects until the second half of 20th century. France and England were major manufacturers of toothbrushes in 19th century, but they were considered luxury articles and regular tooth brushing was not a widespread practice until after the second half of 19th century (Asbell, 1992). Since the 1970s a striking decline in caries experiences has been observed throughout industrialized countries (Brunelle & Carlos, 1990; Shafer et al., 1983). This seems to be related to dental treatment and the introduction of fluoride13 water and toothpaste. Also, the decline in dental caries rates was due to a range of changing social factors that seem to be linked to improvements in general health indicators (Haugejorden, 1996; Nikiforouk, 1985; Shaw, 1985). But in emerging countries the situation is the opposite and high caries rates are associated with malnutrition, absence of health services and poor quality of life (Alvarez, 1988; Campodónico et al., 2001; Heredia & Alva, 2005).
Sugar is derived from a natural grass, this is true. But that natural grass sugar is different than the end product that we use. Sugar cane juice in its natural form comes with added fiber. It is also full of healthy nutrients. If we were to eat it without the processing, we would find that it wasn't so bad for us. The reason being is that sugar juice in the plant is again combined with fiber. Eating it together and in correct portions won't cause you harm, in fact, it can be beneficial:
sugarcane, because it has fiber and nutrients (yes! sugarcane is full of nutrients, and is LOW on the glycemic index when consumed whole!) is a healthy additive to your diet. It has been known to fight viruses like cold and flu as well as having cancer fighting compounds. It is also extremely hydrating, and can balance electrolytes when taken after sports since it has a fair amount of potassium. It is also a mild laxative, and can help clear your body of kidney stones and keep the urinary flow clear. Since sugarcane contains no simple sugars either, it's only when we process it that it becomes unhealthy, and contains ample carbohydrates when consumed whole ...
That's all I could find to support the opposing side for sugar. Every article I looked at showed correlation between curies and increased sugar intake. But the process of increased curies then a "normalization" follows the same path as when we introduced carbs to our diet. If this is the case it lends support to the question I posed in the first section: is there a natural decline and then normalization of health every time we introduce new food products into our diet? I don't know if that is something we can determine, but it is an interesting thought none the less.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)
Simple Carbohydrates and Sugar Act The Same
We need to understand that when talking about sugar or simple carbs, we are talking about all the products, both natural and artificial, that are considered sweeteners. Sugar and simple carbs are intertwined and go hand and hand when we talk about health concerns related to consumption. But, as we discussed earlier, there are a few different types of carbs. The ones we are discussing here are simple carbs. This whole thread, anytime carbs are mentioned, I am just referring to simple carbs. Refined sugar and simple carbs are married and I use the terms in general to refer to both products. They may have different last names, but they are treated by your body the exact same way. Natural or complex carbs are healthy for you to eat in correct portion sizes. It is important you understand the difference.
Sugars, whether natural or added, digest the same way. Enzymes secreted by your small intestine quickly convert sugars into glucose, which is the simplest form of sugar. Glucose enters your bloodstream through intestinal walls and enters cells for fuel, with the help of the hormone insulin. Metabolizing sugar happens rapidly, often giving you a burst of energy, after consuming sugar-rich foods ...
I know how we love to label things. Currently we have 56 different names for sugar and we have 4 classifications of carbs. Two of those carb classifications are just a way to say they are sugars from a different source other than refined sugar, but they are metabolized the same way. There is only two sources of simple carbohydrates that are good for you: fruits and vegetables. The best sources of these two are fresh or frozen, never canned and certainly not as an ingredient within other processed foods.
The rest of the simple carbohydrate world is "fake news". You need to forget about it and stop eating it if you decide that sugar is no good for you. Products such as bread, pasta, cereals, and pastry are not natural sources of carbohydrates. The number one defining factor between real and simple carbs is natural fiber ( and some nutrients). Fruits and veggies have natural fiber built into them that help your body metabolize their sugars at a slower rate. This decreases the chance that you'll gain weight when you eat them in proper daily amounts.
Fake news carbohydrates usually do not have enough fiber in them to slow down the metabolizing process, which means they basically get metabolized as fat. Also, these carbohydrates usually have other sugar mixed right in with them. Normally if you are eating simple carbs, you are eating refined sugar as well. Not to mention the chemicals and additives used for preservation. The only carbohydrates you can trust are ones you make yourself because you can control what ingredients get included.
Your body uses carbohydrates as its main supply of fuel. Once eaten, the body turns carbs into sugar called glucose. Insulin flushes the glucose into your cells, where it becomes energy. If there is extra glucose left over from the process, it is stored as fat ...
The problem is how we metabolize simple carbs or sugars. They don't tell us when to stop eating them. When you eat something that doesn't send a signal to your brain that you are full, you tend to overeat. If you eat too much, the body will use what it can for immediate energy, then store the rest as fat. If you never know you are eating too much, how do you stop eating too much?
The rub is that sugar also gets metabolized in the same fashion as simple carbohydrates. So, all those foods labeled carbohydrates that aren't natural sources (On this earth before we invented them) are really just sugar in disguise. The label is misleading and the ingredients list on the packages are also misleading. Why do we need 56 different names for sugar? Once it passes our lips, it doesn't matter...it all gets metabolized the same way.
Now you are thinking "Fruit has simple carbohydrates in it and is healthy for you. Why is that ok to eat?" Yep, this is correct. But it also has fiber in it. The ratio of fiber to carbohydrates is 1:10. Which means for every 10 grams of carbs there is one gram of fiber included. Guess what the suggested ratio/daily intake of fiber to carbs is? 1:10. That's why natural carbs are almost never an issue. Because they also have fiber to help digest them properly.
Here's the problem with simple carbs. This is why it gets so confusing for everyone. There are 4 main categories with anywhere from 3-6 subcategories in each of them. Now, if you are in the science business, this is helpful. If you are a regular person, this is confusing. I could list all the categories and sub categories, but there isn't really any need. It is as simple as : any carb products that are NOT natural are bad for you unless you make them yourself and have control over the ingredients.
The other thing that happens with both simple carbs and sugar is that they don't send the signals to your brain that you are satiated. Natural carbs and sugars will tell your brain to stop eating once it has enough fuel. That is what fiber helps with as well. It slows down the processing enough so the Leptin can send a signal to the brain saying "Hey, you can stop eating now, we have a big enough energy supply."
Simple carbs and sugars get metabolized faster and don't produce Leptin. Your brain is never told to stop eating and you continue to eat endless amounts of unneeded food. Also, the sugars from these are more addictive than the natural sugars. Which means you are like a crack addict emotionally. Every time you need a "feel good" moment, you will turn to simple carbs/sugar to get it.
Continued....
edit on 4-2-2018 by blend57 because: (no reason given)
Opposing View
Simple Carbohydrates have their place in this world. They are needed and have many benefits. Once a staple in society, they are starting to get a bad rap. But, when used correctly, simple carbohydrates can be very helpful in burning calories and maintaining energy levels.
For high endurance athletes, simple carbs is usually the best choice for long bouts of exercise. For example, a marathon runner who needs to ensure he has enough energy to last through the full race may load up on simple carbs sometime before the run. The reason being: the body will burn through simple carbs first and then once they are depleted turn to other sources of energy. The marathon runner has a better chance of outperforming their opponent by using this as their primary source of fuel.
Research has shown that carbohydrate loading helps to raise muscle glycogen content. It is believed that carbohydrate loading the day or night prior to a long endurance will provide adequate and extra energy to muscles. Although Carbohydrate loading is popular practice; many are unaware of the process and benefits. Carbohydrates are a main fuel source of the body and help in overall muscle use. Glycogen is the main energy source used by muscles and provides energy during exercise and physical activity. A vast number of studies have been conducted on carbohydrate loading; through this research it has been confirmed that when done properly, carbohydrate loading does work. Carbohydrate loading used to increase or elevate muscle glycogen content higher than normally has been shown to increases energy during endurance events. A study conducted in 1996 by Akermark, C et all; examined Swedish hockey players; the players were randomly split into two groups. The athletes were either given a high carbohydrate diet or a regular mixed foods diet. The players who consumed the carbohydrate rich diet showed improvement in overall speed, distance, and time skating compared to that of the players on a regular diet ...
This paper mentions carbohydrates in general, but a few have pointed to simple carbohydrates as a source of quick fuel, especially when you are short on time before a workout. They provide a quick source of glycogen that your body can make and burn as fuel in less time than more complex carbs.
This is also why sports drinks are used by professional athletes. To recover from depletion of water and nutrients after a high performance workout.
Sports drinks have been researched extensively and generally provide an excellent alternative to plain water for hard working athletes. During intensive aerobic exercise, the body’s preferred source of fuel is carbohydrate (rather than protein or fat) due to the efficiency of energy transfer to fatigued muscles. The majority of sports drinks are formulated to deliver carbohydrates, electrolytes and fluids in such a way that will minimize stomach upset and maximize intestinal absorption for delivery of energy to muscles ...
For me all this means is that depending on your activity level, simple carbs may be good to eat. If you are not running marathons or doing triathlons, you probably should stay away from these things (including sport drinks). If you are a serious professional athlete and spend a majority of your time burning calories every day, simple carbohydrates probably would be ok for you. It all depends on who you are whether they are beneficial or not.
With that said, I should notate that all sources in this opposing view section are referring to all simple carbs, even natural ones that have fiber mixed in with them.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)

High Fructose Corn Syrup (HFCS) Origins
It all started with...politics! And I hate to admit that, and don't want to talk about politics, but I'm kind of forced to. Because that is why we consume so much high fructose corn syrup today. Matter of fact, this whole HFCS debacle started way back when Nixon was running for re-election. It started with politics and then branched off from there:
The story begins in 1971. Richard Nixon was facing re-election. The Vietnam war was threatening his popularity at home, but just as big an issue with voters was the soaring cost of food. If Nixon was to survive, he needed food prices to go down, and that required getting a very powerful lobby on board – the farmers. Nixon appointed Earl Butz, an academic from the farming heartland of Indiana, to broker a compromise. Butz, an agriculture expert, had a radical plan that would transform the food we eat, and in doing so, the shape of the human race.
Butz pushed farmers into a new, industrial scale of production, and into farming one crop in particular: corn. US cattle were fattened by the immense increases in corn production. Burgers became bigger. Fries, fried in corn oil, became fattier. Corn became the engine for the massive surge in the quantities of cheaper food being supplied to American supermarkets: everything from cereals, to biscuits and flour found new uses for corn ...
The article goes on to say how the discovery of high fructose corn syrup increased the demand for corn and the width of our waistlines:
By the mid-70s, there was a surplus of corn. Butz flew to Japan to look into a scientific innovation that would change everything: the mass development of high fructose corn syrup (HFCS), or glucose-fructose syrup as it's often referred to in the UK, a highly sweet, gloppy syrup, produced from surplus corn, that was also incredibly cheap. HFCS had been discovered in the 50s, but it was only in the 70s that a process had been found to harness it for mass production. HFCS was soon pumped into every conceivable food: pizzas, coleslaw, meat. It provided that "just baked" sheen on bread and cakes, made everything sweeter, and extended shelf life from days to years. A silent revolution of the amount of sugar that was going into our bodies was taking place. In Britain, the food on our plates became pure science – each processed milligram tweaked and sweetened for maximum palatability. And the general public were clueless that these changes were taking place.
There was one product in particular that it had a dramatic effect on – soft drinks. Hank Cardello, the former head of marketing at Coca-Cola, tells me that in 1984, Coke in the US swapped from sugar to HFCS (In the UK, it continued to use sugar). As a market leader, Coke's decision sent a message of endorsement to the rest of the industry, which quickly followed suit. There was "no downside" to HFCS, Cardello says. It was two-thirds the price of sugar, and even the risk of messing with the taste was a risk worth taking when you looked at the margin, especially as there were no apparent health risks. At that time, "obesity wasn't even on the radar" says Cardello ...
So, this wasn't anything more than a political campaign strategy. Figures, everything leads back to politics. The point is, it was never done for the benefit of your wallet (even though it proved beneficial in that arena), nor was it done for the health and well being of the American people. It was done to win an election supposedly. That was the main reason for the introduction of HFCS into our diets.
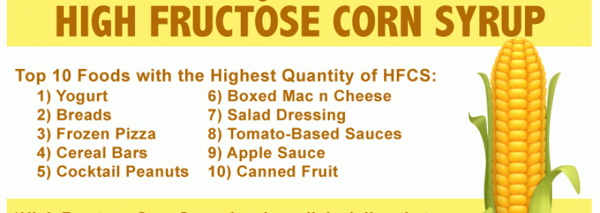
Ever since that point, our high fructose corn syrup use has increased exponentially, being used in over 11,000 products in some way, shape, or form. It's not a hidden fact, everyone knows it. But, it is not something that comes to the forefront of your mind as you are checking ingredients and searching labels. Never mind the fact that the name has changed quite a bit over the years. Most people would never know what to check for even if they were looking. Some of those name changes are:
High-fructose corn syrup, natural corn syrup, isolated fructose, maize (a native word for corn) syrup, and glucose/fructose syrup.
When you are reading the ingredient label, these are some of the names you'll find HFCS listed under. Also, don't think they are found in just your food. You can find this stuff in every thing from toothpaste to cosmetics, vitamins, breath mints, even your non gluten food is made with HFCS. Yep, since gluten intolerance became relevant, the number of products available in the gluten free section of the supermarket rose from 600 items in 2007 to over 1600 in 2011. And it all is made with corn. The damaging affects HFCS has been said to have on your body are as follows:
- Weight Gain
- Cancer
- Fatty Liver, Liver stress
- Increased Cholesterol
- Diabetes
- High blood pressure
- Heart disease
- Leaky gut - When you have this condition, the “net” in your digestive tract gets damaged, which allows proteins (like gluten), bad bacteria and
undigested particles to pass into your bloodstream.
- Increased Mercury intake - Multiple studies have found alarming amounts of mercury in products containing high fructose corn syrup, which can contribute to dangerous mercury poisoning ...
Now, considering that this is in everything we eat, it very well could be the cause of these issues. Who am I to say that it is or isn't. The one thing I think for sure is that it's linked to obesity. Not because it is so much worse than the other sugars we discussed, but simply because we eat too much of it...we eat too much of all types of sugars. Maybe that's really what they are trying to say with all these studies, that all forms of sugar can cause obesity. Which should be obvious to everyone anyways.
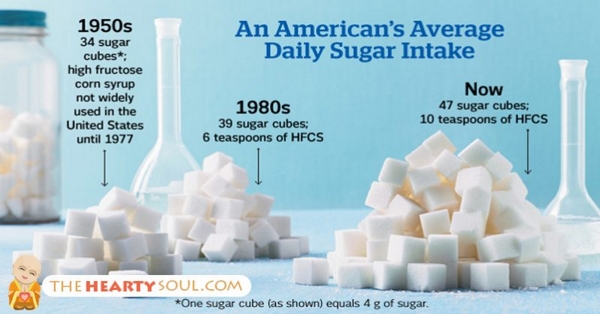
I say that because American diets consists of 25% sugar products. Not just fructose or refined sugar, not just simple carbohydrates and artificial sweeteners (covered next). That is 25% in total. That is a staggering amount of sugar to eat. I also don't know if it is accurate. I think we probably eat way more, but just don't realize it. I don't think that eating sugar is the cause of obesity, but the huge amounts we eat is the cause. And I think we eat the amount we do because we just don't know it's in the food. No one wakes up one day and says "I want to eat 42.5 teaspoons of sugar, let's see what's in the fridge!"
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)
Opposing View
Again, we hear the argument that no direct link can be found concerning HFCS and the health conditions listed above. The argument is that it is no worse for you than table sugar and as such, as long as you are eating it in proper portions, it is just as harmless.
Fructose intake has recently received considerable media attention, most of which has been negative. The assertion has been that dietary fructose is less satiating and more lipogenic than other sugars. However, no fully relevant data have been presented to account for a direct link between dietary fructose intake and health risk markers such as obesity, triglyceride accumulation and insulin resistance in humans. First: a re-evaluation of published epidemiological studies concerning the consumption of dietary fructose or mainly high fructose corn syrup shows that most of such studies have been cross-sectional or based on passive inaccurate surveillance, especially in children and adolescents, and thus have not established direct causal links. Second: research evidence of the short or acute term satiating power or increasing food intake after fructose consumption as compared to that resulting from normal patterns of sugar consumption, such as sucrose, remains inconclusive. Third: the results of longer-term intervention studies depend mainly on the type of sugar used for comparison. Typically aspartame, glucose, or sucrose is used and no negative effects are found when sucrose is used as a control group.
Negative conclusions have been drawn from studies in rodents or in humans attempting to elucidate the mechanisms and biological pathways underlying fructose consumption by using unrealistically high fructose amounts.
The issue of dietary fructose and health is linked to the quantity consumed, which is the same issue for any macro- or micro nutrients. It has been considered that moderate fructose consumption of ≤50g/day or ~10% of energy has no deleterious effect on lipid and glucose control and of ≤100g/day does not influence body weight. No fully relevant data account for a direct link between moderate dietary fructose intake and health risk markers ...
I have to admit, I had a hard time finding a study that showed the opposing view. Most of them are citing that HFCS is a hazard to your health in one way or another. But still, this one does have a valid point: how are the studies being done to show a link to obesity? It seems the argument is that they've based their conclusions on inaccurate surveillance, that the sugars they are comparing them to are not the typical ones used, and they used of unrealistic amounts of HFCS in the studies. Basically accusing the studies of manipulating data to achieve desired results. Which hopefully isn't the case.
In addition, the introduction/development of HFCS helped out the American economy. We began to produce more corn and export it to other nations. We were able to lower the prices of our food, make things cheap and affordable in a time when every penny counted. It gave our agriculture industry a big boost as well. Economically, it was the right thing to do.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)

Artificial Sweeteners Origins Part 1
After we learned how to refine and mass produce sugar, we stumbled onto artificial sweeteners. And when I say we stumbled onto it, we actually did. Saccharin was accidentally discovered in 1879 by a gentlemen that was working on coal tar derivatives. Don't ask me how he managed to get figure out it tasted sweet, but he did. After that in a few decades we have developed a ton of different types and put them on the market.
The development and introduction of the main artificial sweeteners is as follows:
The first artificial sweetener, Saccharin, was discovered 1879. In the beginning, it was primarily used by diabetics. Cyclamate was discovered in 1937 by Michael Sveda. It was blended with saccharin to improve taste. A ban was put on Cyclamate from 1969, but it was eventually allowed back onto the market. In 1965, James Schlatter at Searle discovered aspartame [10]. He was trying to make new ulcer drugs. It was approved for use in 1981 in dry foods only, and then as a general sweetener in 1996 (almost there! just a few more). Neotame was approved in 2002 for use by the FDA, Acesulfame potassium was discovered in 1967, and approved for general use in 2003, sucralose was discovered in 1979 and approved in 1999, and more than 6,000 new products were launched in the United States between 1999 and 2004 ...
Pretty much everything we eat has either refined sugar/simple carbs, HFCS, or artificial sugar in it. There is nothing that has been processed that doesn't have one of these things as an ingredient. Artificial sweeteners, although advertised as a diet substitute for sugar, have been shown to have some major health effects as well. The main one being weight gain:
Intuitively, people choose non-caloric artificial sweeteners over sugar to lose or maintain weight. Sugar provides a large amount of rapidly absorbable carbohydrates, leading to excessive energy intake, weight gain, and metabolic syndrome [15,16,17]. Sugar and other caloric sweeteners such as high fructose corn syrup have been cast as the main culprits of the obesity epidemic. Whether due to a successful marketing effort on the part of the diet beverage industry or not, the weight conscious public often consider artificial sweeteners “health food” [6]. But do artificial sweeteners actually help reduce weight?
Surprisingly, epidemiologic data suggest the contrary. Several large scale prospective cohort studies found positive correlation between artificial sweetener use and weight gain. The San Antonio Heart Study examined 3,682 adults over a seven- to eight-year period in the 1980s [18]. When matched for initial body mass index (BMI), gender, ethnicity, and diet, drinkers of artificially sweetened beverages consistently had higher BMIs at the follow-up, with dose dependence on the amount of consumption. Average BMI gain was +1.01 kg/m2 for control and 1.78 kg/m2 for people in the third quartile for artificially sweetened beverage consumption. The American Cancer Society study conducted in early 1980s included 78,694 women who were highly homogenous with regard to age, ethnicity, socioeconomic status, and lack of preexisting conditions [19]. At one-year follow-up, 2.7 percent to 7.1 percent more regular artificial sweetener users gained weight compared to non-users matched by initial weight. The difference in the amount gained between the two groups was less than two pounds, albeit statistically significant. Saccharin use was also associated with eight-year weight gain in 31,940 women from the Nurses’ Health Study conducted in the 1970s [20]. ...
They are in products you would never guess included them, such as vitamins, toothpaste, mouthwash, breath mints, and, sometimes, even your water. There was a study done on the waste water in Germany which found that artificial sweeteners were present. I know, waste water, but waste water sometimes gets recycled into tap water in some areas. So, depending on the purifying treatment, you could very well be drinking artificial sweeteners without even knowing.
Occurrence of sweeteners in German surface waters
In all German surface waters analyzed, acesulfame,saccharin, cyclamate, and sucralose were detected, which proved the observed incomplete removal in STPs (Fig. 3and Table S7, Electronic Supplementary Material). Sweet-energy levels in the investigated German rivers correspond to STP effluent concentrations when taking into account a dilution approximately between a factor of 10 and a factor of 100.
Acesulfame was found in several samples in concentrations higher than
2μ g/L and, in most cases, occurred in about tenfold higher concentrations than other sweeteners. Saccharin and cyclamate were detected at levels between 50 and 150ng/L in the majority of the river water samples. Findings of sucralose in German rivers were in excellent correlation to the values obtained for Germany in the EU-wide monitoring program [30]. Most samples showed sucralose concentrations between 60 and 8ng/L with only one value exceeding 100 ng/L.Aspartame, neotame, and NHDC were again not detected in any analyzed sample.
Conclusions
The method developed allows the simultaneous extraction and analysis of seven artificial sweeteners from difficult environmental matrices, such aswaste water and surface water. Accurate quantification could be achieved by the use of a deuterated standard and sample dilution. Application of this method to waste water samples, samples obtained from a soil aquifer site, and surface water samples demonstrated incomplete removal of some of these compounds during waste water purification. Due to their use as food additives, the occurrence of artificial sweetener traces in the aquatic environment might become a primary issue of consumer acceptance, especially as the aspect of drinking water quality, which might be negatively influenced by potential metabolites of these trace pollutants, is completely un-known yet ...
Continued...

Artificial Sweeteners Part 2
I can't say for sure if they've done the same testing in the states, I was not able to find any sources on it. I would assume they would get similar results though if they did, as we are one of the largest consumers of artificial sweeteners in the world.
The other health issues associated with artificial sweeteners are:
- Metabolic Syndrome: increased blood pressure, a high blood sugar level, excess body fat around the waist, and abnormal cholesterol levels
- Type-2 Diabetes: risk for developing type 2 diabetes more than doubled for participants in the highest quartile of diet beverage consumption,
compared with non-consumers.
- Hypertension and Cardiovascular Disease: Consuming at least one artificially-sweetened beverage daily significantly elevated risk for hypertension
for women in a number of studies.
- Migraines, change in vision, nausea and vomiting, insomnia/sleep problems, abdominal and joint pains, change in heart rate, depression, memory loss, seizure, and brain cancer/tumors.
Some of these issues are testimonials only and have been reported to the FDA by regular consumers. As always though, the pendulum swings both ways.

Opposing View
Artificial sweeteners were developed/discovered for the very first time in 1879. Although discovered by accident, eventually we found a use for them in helping insulin dependent and diabetics reduce their sugar intake. They were also easier to mass produce than refined sugar, which kept them affordable for purchase/use.
Before the world war, sugar had been pretty expensive. Mainly high class, well to do society members were able to afford it. Artificial sweeteners were around back then, but were thought to be for medicinal purposes instead of general consumption. At the end/during the world war, when women wanted to present more slim, trim figures, that is when artificial sweeteners became mainstream and we eventually were presented with more options to choose from.
Throughout the years, they've gotten some bad press. Supposedly linked to many different health issues and obesity. The problem with that is none of them can be directly linked to any of the health issues that they have tried to link them to. Reported personal accounts to the FDA have not been corroborated through science and so far, all of the real serious issues that have been brought forth have opposing studies that counter the results.
With that stated, the FDA has approved these artificial sugars for consumption. They are said to be GRAS (Generally Regarded As Safe). The way they determine if a GRAS substance is safe is as follows:
How does FDA regulate the use of high-intensity sweeteners in food?
A high intensity sweetener is regulated as a food additive, unless its use as a sweetener is generally recognized as safe (GRAS). The use of a food additive must undergo premarket review and approval by FDA before it can be used in food. In contrast, use of a GRAS substance does not require premarket approval. Rather, the basis for a GRAS determination based on scientific procedures is that experts qualified by scientific training and experience to evaluate its safety conclude, based on publically available information, that the substance is safe under the conditions of its intended use. A company can make an independent GRAS determination for a substance with or without notifying FDA. Regardless of whether a substance is approved for use as a food additive or its use is determined to be GRAS, scientists must determine that it meets the safety standard of reasonable certainty of no harm under the intended conditions of its use. This standard of safety is defined in FDA’s regulations. ...
Which high-intensity sweeteners are permitted for use in food?
Six high-intensity sweeteners are FDA-approved as food additives in the United States: saccharin, aspartame, acesulfame potassium (Ace-K), sucralose, neotame, and advantame.
The ADA and AHA have both determined that artificial sweeteners are safe for consumption as well. Although they caution you to use them responsibly.
By increasing palatability of nutrient-dense foods/beverages, sweeteners can promote diet healthfulness. Scientific evidence supports neither that intakes of nutritive sweeteners by themselves increase the risk of obesity nor that nutritive or nonnutritive sweeteners cause behavioral disorders. However, nutritive sweeteners increase risk of dental caries. High fructose intakes may cause hypertriglyceridemia and gastrointestinal symptoms in susceptible individuals. Thus, it is the position of The American Dietetic Association that consumers can safely enjoy a range of nutritive and nonnutritive sweeteners when consumed in a diet that is guided by current federal nutrition recommendations, such as the Dietary Guidelines for Americans and the Dietary References Intakes, as well as individual health goals. Dietetics professionals should provide consumers with science-based information about sweeteners and support research on the use of sweeteners to promote eating enjoyment, optimal nutrition, and health. ...
None of these organizations see any adverse effects from the use of artificial sweeteners. They have access to and have reviewed the same scientific studies as everyone else. So far, there has been inconclusive evidence to warrant any concern with regards to consuming products made with artificial sweeteners.
Continued...
A Calorie is NOT just a Calorie
So many people think that losing and maintaining weight is as simple as calories in, calories out. And it's ok to think that, because it's true! In the end, that still applies...calories in, calories out is very much the way things work honestly. That's really not even in question. So, good news! If that is what you think, you're right!!!
But there is no such thing as a calorie is just a calorie. There are calories that allow you to perform better than others. They are natural to this Earth designed to help you function at optimum level. Our bodies are used to them, they are what we've been eating for thousands of years, even before the Neolithic Revolution. I'm not going to go into all the technical details about how we adapted to our eating habits/lifestyles. I covered some of that in the first two sections, as well as there's really is no need to do so. Basically all you need to know is: Choose natural foods (value calories) over refined foods (empty calories) and eat them in correct portion sizes. But let's look at it from a calorie in/calorie out viewpoint anyways.
Calories In MINUS Calories Out = Energy Balance
That's the formula, this is the premise:
No matter what kind of food you eat, if your reduce your daily calorie intake (food) and maintain/increase your energy output (exercise) you will lose weight.
Sure, that can happen. And for anyone who wants to count calories and weigh their food everyday, I guess that is a good formula to follow. I really don't want to do that. I don't have the time nor the inclination. It is a pain in the ass and who wants to spend their free time that way? What most people don't realize though, is that if you eat the right kinds of food, you won't need to count calories...your body will do it for you. Yep, your body will tell you when to reduce your food intake, when to increase it, and do all the CICO formulas for you. And all you have to do is eat the right foods, that's really all there is to it.
All food is just an energy source. It supplies your body with what it needs to function during the day. The whole body. That includes your mind, skin, organs, muscles, bones, tendons, etc.. And when you have enough energy to make it through the day, your liver sends a chemical message to your brain telling it that "it's ok, we're good to go, you can stop eating now."
When you use up all that energy or you're getting low, your stomach sends a chemical message to your mind telling it that you need to refuel. So, there is a natural process of CICO being followed....if you eat the right foods. Because not one person is the same as another. We all run at different metabolic rates, burn energy differently. Because of that, we all need a different amount of calories to make it through the day.
That's how it should work and your body wants it to work that way too! That's what it's set up to do. No one is wrong when they say CICO is the process. It is the process and normally how you lose weight. And prior to the invention of GMO, chemically altered, highly processed, sugar infused food...this worked. But in today's world, it isn't so simple. We need to eat smarter in order not to work harder to obtain our weight loss and health goals.
A calorie is no longer a calorie. Now, there are hidden elements within your food. Calories that the body isn't used to processing, calories that don't tell the mind that your full, calories that sometimes increase your hunger instead of satiating it. Calories that aren't easily identifiable and are misrepresented on packaging. Those calories come from sugar and simple carbohydrates.
And, you know the difference if you think about it. It's the difference between a frozen chicken nugget and a piece of chicken. You can eat a ton of chicken nuggets. But normally one chicken breast will fill you up. It's the difference between a fast food burger and a home made burger or french fries versus a baked potato. More often than not, you will consume a larger quantity of fast food/processed food than you will if you eat the natural version of it. You know the difference, there is no science needed in this part, you can tell by the way your body reacts to the food you eat.
Lots of people can sit and eat a whole bag of potato chips. Not many can sit and eat the equivalent to that in natural potatoes. Can you sit down and eat 5-7 natural potatoes in one sitting? Probably not. Yet that is how many potatoes are used in each bag of chips. You have to wonder why it is that you can eat a whole bag of chips. What is the difference?
It is how they make the chips. What they take out and what they put in. The GMO oil they fry them in, the nutrients and fiber they pull out of them and the new stuff they put back in. Remember I said for every 10 carbs you need 1 fiber in order to make your digestive system process the food correctly, in order to make the CICO work.
Potato chips have about 1/2 the fiber (unnatural fiber) per serving as a potato (depending on brand, flavor, and size). Plus, they don't tell you when you are full. So, you're eating more, getting less benefits, and gaining weight. Doesn't make much sense, does it? That's what makes a calorie NOT a calorie. And that is why CICO does NOT work for some people. What a calorie is made of matters.
Continued...

Allergies and CICO
This is just a small section with regards to personal observations around allergies and food. It fits well with the a calorie is not just a calorie section so I thought I would include it here. One of the primary reasons I have trouble supporting the a calorie is just a calorie theory is because of allergies. Many times, one of the first areas a doctor will look at with regards to allergies is your food. Often, they will adjust your diet to very basic foods and then slowly introduce more options until the food source that is causing your issues is found.
To me, if a calorie is just a calorie, there would be no allergic reactions to anything that you eat. The fact that we have food allergies kind of ruins the "calorie is just a calorie" portion of the CICO theory. Along with all the other health issues people develop from their eating habits. Alcohol is a caloric drink. If a calorie was just a calorie, there would be no consequences to drinking huge amounts of it. Sugar wouldn't cause diabetes, there would be no peanut allergies, no lactose intolerant people...we would all be able to eat and drink whatever we wanted.
But we can't. And a lot of times the solution to many skin/food allergies is to cut something from your diet. Which means that what you eat definitely is metabolized according to what's in it. An allergy to something also means that your body can't metabolize/burn it effectively. So that leads me to beleive that every calorie has an impact on our system and how our bodies perform. Which also tells you that a calorie is not just a calorie. It is important for people who are allergic to peanuts not to eat them. It is important for people who have liver damage not to drink. Which means some calories definitely have more value than others.
Continued...
Sugar/carb Addiction Part 1
There have been studies that show sugar/carb consumption is just as addictive as coc aine. The effects on your body and mind are exactly the same eating sugar as it is snorting a line of coke. The addiction is so severe that you go through withdrawals when you are unable to consume sugar.
There are basically 4 signs that you have an addiction to sugar. Binging, withdrawal, craving, and sensitization. Many studies have shown that sugar/carb consumption follows these steps.
After a month on this intermittent-feeding schedule, the animals show a series of behaviors similar to the effects of drugs of abuse. These are categorized as “bingeing”, meaning unusually large bouts of intake, opiate-like “withdrawal” indicated by signs of anxiety and behavioral depression (Colantuoni et al., 2001, 2002), and “craving” measured during sugar abstinence as enhanced responding for sugar (Avena et al., 2005). There are also signs of both locomotor and consummatory “cross-sensitization” from sugar to drugs of abuse (Avena et al., 2004, Avena and Hoebel, 2003b) ...
Recent findings Recent work on food use disorders has demonstrated that the same neurobiological pathways that are implicated in drug abuse also modulate food consumption, and that the body's regulation of food intake involves a complex set of peripheral and central signaling networks. Moreover, new research indicates that rats can become addicted to certain foods, that men and women may respond differently to external food cues, and that the intrauterine environment may significantly impact a child's subsequent risk of developing obesity, diabetes, and hypercholesterolemia ...
Let's start with binging. I will compare drug symptoms to sugar/simple carbs symptoms as I work my way through each sign of withdrawal. While you're reading maybe you can assess whether or not you've experienced these symptom in your own life when you've reduced/eliminated sugar/simple carbs from your diet for a time.
Binging
Binging is caused by a strong desire to satiate your need for...not a food, but a feeling. Inside our body there is a bunch of chemical reactions or if/then scenarios going on. For example, if you eat something sugary, then your body/mind will feel euphoric for a bit. You feel more energetic, alert, and happier. The same goes with drugs. Both products, sugar and drugs, have the same end result. How it happens is a lot of science mumbo jumbo, but basically you intake the substance, a reaction occurs, and your brain gets overloaded with "feel good" chemicals.
Let's say that you spend a month eating the same amount of carbs/sugars. Your body gets used to that euphoric feeling and expects it to happen pretty much at the same time/frequency every day. And, for some reason, you have to delay the intake one day. When you are able to ingest the substance, you're probably gonna binge eat it. It is the delay in gratification that will cause you to eat more. From the moment your mind is deprived of it, it starts sending signals to your body to seek it out.
There is also another way you binge eat. Once your body gets accustomed to a certain dose of food (used to the chemicals it sends to the brain), it will start asking for more. After a certain time the dosage is just not as effective as it once was. So, your brain, being smart and logical, tells you to increase the dosage in order to maintain the level of euphoria it's used to. This cycle continues on until you are ingesting way more of the substance than your body can handle. Even if your body starts to become damaged by the amount of the product your ingesting, the brain still wants you to increase the supply...the addiction is more important than your health.
In the beginning, you may have only eaten one candy bar. Now, your eating two to three candy bars a day. Same goes with carbs. You might have started out eating a small fry from McDonalds, now you're super sizing them. This is the start to binging. Over time you will began to eat more and more at every meal. And, you will eat more meals throughout the day. All NOT because you're hungry, but because of a feeling. Here is the definition of binging for a drug addict:
As a person desires the sense of euphoria that accompanies a certain drug and finds that after their first use that taking the same amount does not result in the sense of pleasure that the first use did, they begin to take more and more in hopes of replicating the initial feeling. Depending on the drug, this binge can take place over a matter of hours, or as long as several days ...
And the definition for food binging:
The Diagnostic and Statistical Manual of Mental Disorders (ed. 4) defines binge eating as a series of recurrent binge episodes in which each episode is defined as eating a larger amount of food than normal during a short period of time (usually within any 2-h period)
To put it simply, people usually binge on highly palatable energy-rich food. These foods are typically high in fats, sugars, or often both (8,9). Binge episodes often involve consumption of bread or pasta, followed in frequency by sweets, fatty foods, or salty snacks (10). Individuals with a preference for bingeing on sweet foods tend to binge more frequently ...
Notice some similarities? There are plenty and as we move forward to the next section, you will see that drug & sugar addiction mirror one another. I also hope you will be able to tell if you have a sugar addiction or not. Note that both of these addictions are caused by the same thing...emotions. They are chemical reactions in the brain, yes, but we desire the emotional response we feel from those chemical reactions. Dopamine floods the brain, the amygdala gets activated, the hypothalamus goes into action and for a few short moments (usually 30 or less), we feel better emotionally. This process is almost immediate for both coc aine and sugar, a quick, short high, followed by a long withdrawal.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)

Part 2
Withdrawal
This is one of the worst parts of any addiction. Once you realize that you're addicted to something and then try to quit. The withdrawal symptoms can be unbearable. If you go cold turkey with drugs, as the days progress the symptoms get worse. Oddly enough, it is reported that the same thing happens with sugar/simple carbs. The withdrawal process can become overwhelming and, at a certain point, you end up succumbing to the urges and binge.
Many drug users have reported the effects/symptoms of withdrawal. It is well documented. I chose coc aine for comparison because that is what sugar addiction is supposed to emulate.
Symptoms of coc aine withdrawal ...
- Difficulty concentrating
- Fatigue or exhaustion
- Anhedonia, or the inability to feel pleasure
- Inability to experience sexual arousal
- Depression or anxiety
- Physical symptoms, such as chills, tremors, muscle aches, and nerve pain
- Suicidal thoughts or actions
- Increased craving for coc aine
- Increased appetite
- Vivid, unpleasant dreams or nightmares
- Slowed activity, or physical fatigue after activity
- Slower thinking
- Restlessness
The following is/are the symptoms reported for sugar withdrawals ...
- Headaches
- Bloating
- Nausea
- Muscle aches
- Diarrhea
- Fatigue
- Hunger
- Anxiety
- Depression
- Cravings
- Chills
I've bolded the symptoms that mimic the coc aine withdrawal ones for ease of comparison. Pretty close match up to one another. Headaches, bloating, nausea, and diarrhea could also be symptoms of coc aine withdrawal. I am unsure if they are grouped under the Physical symptoms, such as chills, tremors, muscle aches, and nerve pain section or not. I left them un-bolded because they weren't specifically stated to be coc aine withdrawal symptoms.
Realistically, if the sugar/simple carbs symptoms are true, so far we have what seems like potentially addictive substances. What we have to take into consideration is the length of time that these symptoms take to develop. With coc aine, they start within a few hours, become more severe as time goes by, and take weeks/months to diminish (up to six months). Sugar follows the same cycle, but it is not as severe. The withdrawal period is shorter ( two - four weeks) and the ability to recover and stay recovered is greater. We are talking months (coc aine) versus weeks (sugar/carbs).
The difference in recovery/withdrawal times is significant. The strength of a sugar/simple carb addiction should be just as severe as a coc aine one, based upon the fact that we have been eating sugar/simple carbs since we were born. The longevity of an addiction matters, as does the intensity or dosage. Sugar/simple carbs are the most used "drug" out there. The dosage is 18 spoonfuls for an average adult a day. Cocaine is usually a couple of lines. Potency is important as well. Both drugs go straight to your brain. It is the first place glucose is sent to for the brain to use as energy. This means that maybe, if sugar was a drug, it would be more addictive than coc aine and the withdrawal symptoms should be as severe in both longevity as well as intensity. That does not appear to be the case.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)

Part 3
Craving
Craving should actually be first on this list. Once you introduce your body to a new "drug", craving is the first indication that you need your "fix". After that comes withdrawal and binging. Craving is a chemical process as well. When you take a drug or eat something pleasurable, the brain sends signals throughout the reward system network. Usually, if you like the taste/feeling, the brain says that this is something it should try again. That strengthens the addiction and also will cause you to crave more. But there are new findings that possibly point to other parts of the brain being involved with craving. One is the hypothalamus.
Cravings will become more intense as the minutes/hours go by. At first maybe just a thought: "I should eat a cookie." As the moments pass, you start to get withdrawals and also, your craving intensifies. Ever try not to eat a sweet and you end up eating everything else you can find in the fridge and then still eat the sweet? That is your body/mind seeking out its fix. Your brain won't be satisfied until it gets the reward it desires. Once you eat the sweet, everything stops. The cravings, withdrawals, urge to binge eat...everything goes back to normal. Until your body is ready for its next fix.
For coc aine addicts, the cravings are a bit more intense. It seems like they have a couple different times of very strong cravings after they use. The first being the 1-3 hours immediately after use when they are coming down. The second being 1-2 days after their initial use (depending on the amount and frequency of use). It is a psychological craving for coc aine addicts. This is/has been noted in several studies.
The researchers hooked the rats on coc aine by delivering intravenous doses when the rodents pushed a lever in their cages. The researchers then made the rats quit cold turkey by replacing the coc aine with a saline solution. After a week, the animals stopped pressing the lever seeking a coc aine fix.
The researchers then sought to trigger a relapse by electrically stimulating two parts of the brain.
One was the "reward" or "liking" center that registers the high from using the drug -- a brain pathway that involves a chemical called dopamine.
The other was in the hippocampus region of the brain, which is associated with memory and involves glutamate, an entirely different brain chemical. This region appears to register the memory of a drug's effects and the craving for it, Vorel said.
Stimulating the hippocampus caused an intense craving for coc aine, the study found. The rats repeatedly pressed the lever that previously had delivered coc aine ...
The new theory is that psychological dependencies are related to the memory section of the brain. Which means your brain is remembering what it felt like and the effects the drug had on you at the time. The trigger could be anything from being in the same room you took the drug in previously to a smell. That memory could lead to the memories of being high and thus create a strong, insatiable urge to obtain more... a craving. For all intense and purposes, it is an emotional dependency.
There are three regions of the of the brain – the hippocampus, insula, and caudate nucleus – that appear to be activated during food-craving episodes. What’s most interesting, however, is that these are the areas of the brain responsible for memory and sensing pleasure.
This makes perfect sense if you think about it, because when do you notice those intense food cravings coming up? For most of us, research says, cravings get intense when we’re stressed or anxious. Memory-related food cravings are indeed that: Our bodies are yearning for the good times and the good feelings of the memory that’s associated with a particular food ...
The memory theory also is associated with food cravings. Although in both cases dopamine release and over active hypothalamus gland occur. This is what leads me to believe that both addictions act the same way regarding cravings and also, that there is/may be a primary and secondary system of craving. Almost like your body has several ways to seek out what it wants to satisfy its needs.
Continued...
Part 4
Satiation
Satiation is the final symptom of an addiction. It means your body builds up a sort of immunity to your normal dosage of drugs. For instance, if you were a once a day user, after a time your mind will start to numb against the effects of the drug and, in order to get the same level of "high", will require more of the drug to do the job. Eventually you will become a twice a day user, then 3 times a day, so on and so forth. You will began to use more and more to get the same high that you obtained from your original dosage.
This becomes a problem because it is coupled with the other three addictive behaviors: craving, binging, and withdrawal. You become like a Ouroboros, stuck in the continuous cycle unless you somehow break it or until death. Your body starts to degrade (internally and externally), you lose your faculties, organs start to fail, and you are stuck on the slow train to the final destination.
I mention all that because we need to realize that sugar/simple carbs, although addictive, can not be compared in strength nor intensity to a drug habit. It has some of the same qualities, but to break the habit or control the intake, for most people, is not as difficult. I don't want to minimize the accomplishments of a recovering drug user. They deserve to be recognized for their strength and courage to face every day with a clean body and clear head.
I also don't want to scare a sober person into thinking that they are unable to break their sugar habit. So, although there are some similarities, and you can see them clearly, for most people sugar is not going to be such a hard thing to eliminate from their diet. It takes about seven to ten days to break the sugar habit. The withdrawals are over within a few days. That is not the case for a drug addict.
So, there you have it. The 4 symptoms of a drug addict. A sugar/carb addict has those same symptoms. How do you figure out if you are one? Quit sugar for a few days and look for the signs. There really is no other way to find out as sugar/carbs aren't listed as or treated like a drug. Even though they are just as addictive.
Continued...

Opposing View
Sugar/simple carbs has never been proven to be addictive. In case studies, there have been correlations made, but none of it has been conclusive. If you take for instance the studies done with mice, the brain of a mouse is much different than that of a human being. The connections and reward areas react/connect differently. Therefore, in studies where mice were utilized, although there are hints of food addiction, it can only be theorized as to how the effects of sugar addiction in mice would mimic the effects of addiction in a human being.
The authors found that, while sugar may seem addictive instinctively, the scientific literature is lacking substantial evidence that this is true. One reason for this is that different areas of the brain are activated in rodents when they crave food compared to when they crave drugs. While both types of cravings activate the nucleus accumbens (a brain region associated with motivation and the reward system) they activate different parts of the nucleus accumbens. Another reason is that, when rats obtain the desired sugar or drugs, their brains release dopamine, a chemical which is important in motivation and reward; however, this dopamine release quickly returns to its original levels after repeated administrations of sugar, but not for coc aine. Additionally, in many studies claiming to find sugar addiction in rodents, researchers pre-select animals for the study which already have a strong response to sugar. Furthermore, the addiction-like behavior only occurs under very specific experimental conditions, such as food deprivation. “It is important to be aware that these studies were conducted under conditions that do not resemble our typical environments,” says Margaret Westwater, the lead author on the study ....
Because of lack of conclusive evidence, so far, sugar/simple carbs has not been proven to be addictive. Take into consideration the fact that the mice were chosen because they already had addiction-like behavior, and the studies were done under very stringent conditions, such as food deprivation. These two variables alone would manipulate the results of any study.
The other factor is that rats don't have the same sociological pressures we do as humans. They don't have peer pressure or emotional childhood trauma that they wish to forget or numb themselves to for a bit. Rodents have only one thing that drives them when it comes to eating...that is eating itself. A natural instinct to forage for and consume food. Although they do have dopamine release when they eat, it is not processed in the same way (emotionally and physically) as humans process it. Therefore human addiction cannot be determined through studies done on mice/rats.
Personal testimonials of addictive like behaviors when weaning oneself off of sugar/carbs cannot be verified nor can the addictive behaviors be pin pointed to sugar use alone. Without knowing the exact diet and eating habits/health/allergies of an individual both before and after the discontinued use of sugar, there would be no way to know if sugar was in fact the main reason that individuals were having withdrawal symptoms.
In the limited studies done on humans, there is also no way to ensure that each participant is eating the exact diet that is selected for the study. Without having the person being monitored 24/7 in a lab type setting, you wouldn't be able to have the needed control over their eating habits. What the participant may in fact deem as an acceptable controlled diet choice may not be within the parameters of the study. Therefore, any studies done outside a lab and without 24/7 supervision are inconclusive and flawed.
Whether you believe these points to be true or not is up to you. They are just counter points to the sugar/ simple carbs addiction argument. What you derive from each side of the argument is up to you. I do beleive that sugar/carb addiction is real in the sense of the emotional attachment we derive from food and taking into consideration that there are two types of triggers: memory related and chemical reaction. The memory related trigger is where I think food may qualify as an addiction. As we use all of our senses when we eat and associate food with good/bad experiences.
For instance, everyone has that "one thing" that their mom used to make for them when they were children and brings back happy memories. It tends to be a favorite food even when we reach adult hood. Everyone also has that one thing that they can no longer eat due to poor experiences such as when you ate a taco after a full night of drinking and that is what you tasted when you got sick the next morning. You will not eat that food ever again, or at least not for a very long time afterwards.
This is how I see the sugar/simple carbs addiction working. Such strong memories associated with it because of not only the reinforcement of the memories, but the utilization of all of our senses when we eat. But that could go for any food that we eat, not just carbs/sugar.
Artificial sweeteners have been said to be addictive too. But to me these thoughts are solely based on senses. The enhanced flavor/taste of artificial sweeteners create such a strong taste memory that we tend to favor the flavor. Some artificial sweeteners are up to 3000 times the sweetness of sugar. But they do not trigger dopamine release like sugar/simple carbs. Therefore, if they are addictive, it seems like it would be through the taste buds only. There have also been no concrete studies that support artificial sweetener addiction that I was able to find. I did find some that supported other areas of concern though.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)
Keto Diet
I can't really look at the benefits/disadvantages of sugar/simple carbs without going into some detail about the Keto diet. The new craze to restore your mind and body back to a healthy, trim, and energetic state. I am, at this point, on the line as to whether or not I think this diet is one that I would enjoy. Yet, I feel that the next two sections are important in evaluating the health concerns of sugar/simple carbs intake. I will be comparing Gluten Intolerance symptoms to the Keto diet cures. Hopefully we will see how they relate to one another.
Keto is sometimes referred to as the Ketogenic diet. It was/is a diet used to treat epilepsy in children. The plan is based on eating high fat, moderate protein, and low carbs food. You start off by fasting for a couple of days to get yourself in "ketosis". Then you are allowed 5-20% carbs, no sugar, high fat, and moderate protein as your daily intake. This is important as it is a testament to how getting rid of sugar could help you. If any diet would prove that sugar is not good for you, this one should.
It is thought to help you change your bodies habit of burning glucose for energy to burning ketones for energy instead. The fasting clears your body of any left over glucose, and allows it to start burning ketones from what you eat going forward.
The following is a study done that shows positive effects of Keto on obese patients.
PATIENTS AND METHODS: In the present study, 83 obese patients (39 men and 44 women) with a body mass index greater than 35 kg/m2, and high glucose and cholesterol levels were selected. The body weight, body mass index, total cholesterol, low density lipoprotein (LDL) cholesterol, high density lipoprotein (HDL) cholesterol, triglycerides, fasting blood sugar, urea and creatinine levels were determined before and after the administration of the ketogenic diet. Changes in these parameters were monitored after eight, 16 and 24 weeks of treatment.
RESULTS: The weight and body mass index of the patients decreased significantly. The level of total cholesterol decreased from week 1 to week 24. HDL cholesterol levels significantly increased, whereas LDL cholesterol levels significantly decreased after treatment. The level of triglycerides decreased significantly following 24 weeks of treatment. The level of blood glucose significantly decreased. The changes in the level of urea and creatinine were not statistically significant.
CONCLUSIONS: The present study shows the beneficial effects of a long-term ketogenic diet. It significantly reduced the body weight and body mass index of the patients. Furthermore, it decreased the level of triglycerides, LDL cholesterol and blood glucose, and increased the level of HDL cholesterol. Administering a ketogenic diet for a relatively longer period of time did not produce any significant side effects in the patients. Therefore, the present study confirms that it is safe to use a ketogenic diet for a longer period of time than previously demonstrated ...
This next one shows that there is no difference between a Keto diet and a high carb diet.
Design: Seventeen overweight or obese men were admitted to metabolic wards, where they consumed a high-carbohydrate baseline diet (BD) for 4 wk followed by 4 wk of an isocaloric KD with clamped protein. Subjects spent 2 consecutive days each week residing in metabolic chambers to measure changes in EE (EEchamber), sleeping EE (SEE), and RQ. Body composition changes were measured by dual-energy X-ray absorptiometry. Average EE during the final 2 wk of the BD and KD periods was measured by doubly labeled water (EEDLW).
Results: Subjects lost weight and body fat throughout the study corresponding to an overall negative energy balance of ∼300 kcal/d. Compared with BD, the KD coincided with increased EEchamber (57 ± 13 kcal/d, P = 0.0004) and SEE (89 ± 14 kcal/d, P < 0.0001) and decreased RQ (−0.111 ± 0.003, P < 0.0001). EEDLWincreased by 151 ± 63 kcal/d (P = 0.03). Body fat loss slowed during the KD and coincided with increased protein utilization and loss of fat-free mass.
Conclusion: The isocaloric KD was not accompanied by increased body fat loss but was associated with relatively small increases in EE that were near the limits of detection with the use of state-of-the-art technology
...
The personal testimonies to how this has worked for people have been positive. All you have to do is Google Keto Diet and you will find thousands of people telling you how great it is. But, you can do the same thing with negative results as well. It is all about what you put into the search bar. And before someone starts thinkin "hey, she's ditching on the keto diet!", no, I'm not. I think there is a need for this diet just as there is a need for some other ones. I'm just not sure it is one that I need to use for my body type. I'm happy for all of those people who've been successful! If this is what works for their individual body composition, that is all that matters!
What I would like to focus on with the Keto diet more so than weight loss and the outer appearance benefits of it is the physiological effects that Keto has on you. This is where the "gold" is with this diet according to many. And this is also how we will be able to determine if Keto (the no sugar diet) is proof how bad sugar is for you.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)
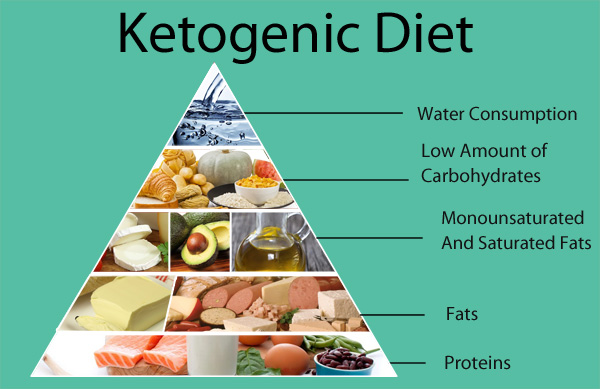
Keto Part 2
Looking at the positive side effects from Keto will cause you to want to ditch your regular diet and try it immediately. The main ones are listed as follows:
- Increased memory/cognition/clarity
- Less Migraines
- Seizure control
- Arthritis
- Eczema/Psoriasis/Acne
- Improved Kidney Function
- Gout
- Improved Energy levels
- Bloating /Improved Digestion/IBS
- Acid Reflux
- Diabetes
- Obesity
- Metabolic Syndrome
I wanted to give a complete list as to what it "cures" so that when we look at the next subject you will be able to compare the two. These cures are personal testimonies mostly, by everyday people that have ditched their normal high carb, sugar infused diet for the keto no sugar diet.
I think that one of the other things that we need to mention that shows a possible correlation between sugar and drug like symptoms is what these dieters call the Keto Flu. Not all of the people who switch to Keto have experienced it, but it does seem like it is indicative of sugar withdrawal. As we just came out of the "is sugar a drug" section, I thought maybe it would be important to share. The Keto flu symptoms reported are as follows:
- Sugar cravings
- Dizziness
- Brain fog
- Irritability
- Poor focus and concentration
- Stomach pains
- Nausea
- Confusion
- Muscle soreness
- Insomnia
It should be noted as well that these symptoms tend to take 1-3 weeks to dissipate and that, although the symptoms are said to be from carb withdrawal, Keto allows 20% carbs. So, more than likely, these symptoms are occurring from simple carbs/sugar withdrawal, which Keto allows zero of in your diet. I've bolded the symptoms that match up with drug withdrawal and sugar withdrawal for convenience of comparison.
Continued...
edit on 4-2-2018 by blend57 because: (no reason given)
new topics
-
Ukraine Style war would mean UK forces would be done in 6 months
World War Three: 17 minutes ago -
So Many Governments teetering
World War Three: 36 minutes ago -
Why Pardon Hunter ? Why risk the fallout?
Political Issues: 1 hours ago -
Disney’s Snow White | Official Trailer | In Theaters March 21
Movies: 3 hours ago -
UnitedHealthcare CEO Brian Thompson shot dead in Midtown Manhattan, masked gunman at large
Other Current Events: 3 hours ago -
More NY Justice System Corruption
Social Issues and Civil Unrest: 8 hours ago
top topics
-
More NY Justice System Corruption
Social Issues and Civil Unrest: 8 hours ago, 17 flags -
Would Democrats Be in Better Shape if They Had Replaced Joe Biden with Kamala Harris in July 2024.
US Political Madness: 15 hours ago, 7 flags -
UnitedHealthcare CEO Brian Thompson shot dead in Midtown Manhattan, masked gunman at large
Other Current Events: 3 hours ago, 7 flags -
Disney’s Snow White | Official Trailer | In Theaters March 21
Movies: 3 hours ago, 3 flags -
Why Pardon Hunter ? Why risk the fallout?
Political Issues: 1 hours ago, 0 flags -
So Many Governments teetering
World War Three: 36 minutes ago, 0 flags -
Ukraine Style war would mean UK forces would be done in 6 months
World War Three: 17 minutes ago, 0 flags
active topics
-
Salvatore Pais confirms science in MH370 videos are real during live stream
General Conspiracies • 99 • : BeyondKnowledge3 -
The Final Experiment is Scheduled for December 2024. Will it Finally Answer the Question?
Science & Technology • 35 • : KnowItAllKnowNothin -
Ukraine Style war would mean UK forces would be done in 6 months
World War Three • 1 • : andy06shake -
So Many Governments teetering
World War Three • 3 • : crayzeed -
UnitedHealthcare CEO Brian Thompson shot dead in Midtown Manhattan, masked gunman at large
Other Current Events • 24 • : asabuvsobelow -
Elon Musk to Make Games Great Again - XAI_GAMES Announcement Incoming.
Video Games • 26 • : KnowItAllKnowNothin -
Map of all wars in history for 2500 years
World War Three • 48 • : stu119 -
Biden pardons his son Hunter despite previous pledges not to
Mainstream News • 144 • : stu119 -
Why Pardon Hunter ? Why risk the fallout?
Political Issues • 7 • : asabuvsobelow -
Could Biden pardon every illegal alien
Social Issues and Civil Unrest • 27 • : nugget1