It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

Quarantine, West Africa: EBOLA UPDATE
page: 2share:
We are bringing back ebola patients to their home countries!
Now I know they need to have the chance to say bye to their families but why do we all have to die for that purpose?
I may sound like a cruel person, Ican tell you I am not but tbh I don't feel like dying because the terminal people have to say bye to family..
Whhy arent we sending their families to africa? (F THEY DARE, im sure the dont so why do we have to put up against this?)
Now I know they need to have the chance to say bye to their families but why do we all have to die for that purpose?
I may sound like a cruel person, Ican tell you I am not but tbh I don't feel like dying because the terminal people have to say bye to family..
Whhy arent we sending their families to africa? (F THEY DARE, im sure the dont so why do we have to put up against this?)
a reply to: HellaKitty89
Since its discovery in 1976, Ebola has been at the CDC in Atlanta, Fort Dettrick in Maryland(?) and most every other level 4 bio-lab on the continent. ...and it's not the worst pathogen we've got - either in our labs - or in our water, soil and air.
Not to say it's not dangerous, but this new sub-clade is very, very different from standard Ebola. And it looks like it just might have come from our labs - and sent to Kenema Hospital in Sierra Leone and the Irrua Hospital in Nigeria. Check out the VHFC - and the "Ethics" constraints:
Since its discovery in 1976, Ebola has been at the CDC in Atlanta, Fort Dettrick in Maryland(?) and most every other level 4 bio-lab on the continent. ...and it's not the worst pathogen we've got - either in our labs - or in our water, soil and air.
Not to say it's not dangerous, but this new sub-clade is very, very different from standard Ebola. And it looks like it just might have come from our labs - and sent to Kenema Hospital in Sierra Leone and the Irrua Hospital in Nigeria. Check out the VHFC - and the "Ethics" constraints:
Molecular Diagnostics for Lassa Fever at Irrua Specialist Teaching Hospital, Nigeria: Lessons Learnt from Two Years of Laboratory Operation
……..The study was classified as a service evaluation and granted exemption from ethical review by the Research and Ethics Committee of ISTH. …….Service evaluation is exempt from ethical review according to the National Code of Health Research Ethics, National Health Research Ethics Committee, Federal Ministry of Health, Nigeria.
About the Viral Hemorrhagic Fever Consortium
The Viral Hemorrhagic Fever Consortium was established in 2010 as a result of several multi-year grants and contracts awarded to Tulane University by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health (NIH), …..The Consortium is a collaboration between …..the Kenema Government Hospital (Sierra Leone), the Irrua Specialist Teaching Hospital (Nigeria) and various other partners in West Africa. More information teachingis available at www.vhfc.org .
Liberia Declares State of Emergency as Ebola Toll Rises
State of emergency declared in Liberia
The state of emergency allows Liberia’s government to curtail civil rights and to deploy troops and police to impose quarantines on badly affected communities to contain an epidemic that has struck four west African nations.
Liberia, Sierra Leone Race To Enforce Ebola Quarantine
….Underscoring desperate attempts to stop the disease, troops in full combat gear deployed in the rain to block people traveling to Liberia's capital from rural areas hit by Ebola. Liberian President Ellen Johnson Sirleaf declared a national state of emergency, and officials said Thursday that no one with a fever would be allowed in or out of the country.
In Sierra Leone, military forces also deployed as part of "Operation Octopus" which officials said was aimed at preventing "the unauthorized movement of Ebola-infected persons."
…Experts warned that extreme measures risk driving patients and their families further underground.
….Sirleaf justified the 90-day state of emergency ….She warned that some civil liberties could be suspended. By Thursday, soldiers were already restricting movements on the roads to Monrovia, witnesses said. Some soldiers were deployed to the crossroads town of Klay, about 25 miles (40 kilometers) west of Monrovia in an effort to stop people from three Ebola-infected counties from coming closer to the capital.
The capital already has been hit by the virus, with bodies abandoned in the streets. Relatives are hiding feverish patients at home for fear if they are brought to isolation centers and don't have Ebola, they will end up contracting it anyway.
National Health Workers Association President Joseph Tamba said the state of emergency is necessary. But he says people should have been given advance notice to buy food ahead of the movement restrictions.
The Centers for Disease Control and Prevention (CDC) has raised their emergency response to the Ebola outbreak to level 1.
This is the highest level of emergency response at the CDC and, according to an agency spokesperson, it has been activated because of the surge of personnel being sent into the affected countries.
…According to the CDC, level 1 is “all hands on deck.” The CDC has only been to level 1 three times in the history of the emergency operations center, which opened in 2003. Previously, it was activated for Hurricane Katrina in 2005 and the H1N1 influenza outbreak in 2009.
edit on 7/8/14 by soficrow because: (no reason given)
a reply to: soficrow
I really dont know much about this kind of diseases, but reading the articles some say those four countries and its citizens are doomed to die because they not reporting themselves or their ill family members in and we are next if these countries will not be on lockdown?
My english is rather good, but reading and understanding news articles is somehow difficult, Iam sory
I really dont know much about this kind of diseases, but reading the articles some say those four countries and its citizens are doomed to die because they not reporting themselves or their ill family members in and we are next if these countries will not be on lockdown?
My english is rather good, but reading and understanding news articles is somehow difficult, Iam sory
a reply to: HellaKitty89
They're not all doomed to die - the death rate is about 50%, but some clinics are saving 75% of their patients in West Africa. Most Ebola infections and deaths happen in hospitals. If this Ebola strain came to the US, the death rate would be much, much lower than 25% - still not good, but a whole lot better.
People are talking a lot of trash for 2 main reasons:
1. To win the coming US election - Obama's competition wants everyone to think he's a failure (at everything, including this).
2. To hide the truth - It sure looks like the US Military and its partners created and released this Ebola, either accidentally or on purpose, from Kenema Hospital (where Sierra Leone, Guinea and Liberia all meet), and from the Irrua Specialist Teaching Hospital in Nigeria.
They're not all doomed to die - the death rate is about 50%, but some clinics are saving 75% of their patients in West Africa. Most Ebola infections and deaths happen in hospitals. If this Ebola strain came to the US, the death rate would be much, much lower than 25% - still not good, but a whole lot better.
People are talking a lot of trash for 2 main reasons:
1. To win the coming US election - Obama's competition wants everyone to think he's a failure (at everything, including this).
2. To hide the truth - It sure looks like the US Military and its partners created and released this Ebola, either accidentally or on purpose, from Kenema Hospital (where Sierra Leone, Guinea and Liberia all meet), and from the Irrua Specialist Teaching Hospital in Nigeria.
I find interesting that now they are "quarantine" the infection areas, but no before Ebola was brought to the US and probably in other countries.
I guess my conspirators mind can not take this news with a happy face.
Now that ebola is a "global thread" vaccinations and treatments needs to be pursued, also every country gets to get ready for a possible pandemic.
Money, money, money, profits, profits, profits.
I guess my conspirators mind can not take this news with a happy face.
Now that ebola is a "global thread" vaccinations and treatments needs to be pursued, also every country gets to get ready for a possible pandemic.
Money, money, money, profits, profits, profits.
a reply to: loam
The time for quarantine was January-February when Ebola first emerged in Kenema Hospital patients, in Guinea and Liberia, as well as Sierra Leone (and maybe Mali). Now, when it's far, far too late, no one can leave Kenema. Then there's Nigeria, the other hospital-related epicenter and outbreak that's been totally covered up - Sawyer is being blamed for bringing Ebola to Nigeria but I call bs - it started in Nigeria's Irrua Specialist Teaching Hospital with the 'research' arm.
April 1, 2014
July 31, 2014

The time for quarantine was January-February when Ebola first emerged in Kenema Hospital patients, in Guinea and Liberia, as well as Sierra Leone (and maybe Mali). Now, when it's far, far too late, no one can leave Kenema. Then there's Nigeria, the other hospital-related epicenter and outbreak that's been totally covered up - Sawyer is being blamed for bringing Ebola to Nigeria but I call bs - it started in Nigeria's Irrua Specialist Teaching Hospital with the 'research' arm.
April 1, 2014
July 31, 2014
No one can leave Kenema
Ebola Frontline: Sierra Leone’s Ebola Epicenter is On Lockdown
When President Ernest Bai Koroma announced a State of Emergency on July 30, many Sierra Leonians hoped that it would mean the government would finally get a handle on the unprecedented Ebola outbreak. However, no one knew until early this morning that for some, this state of emergency meant they were trapped in the epicentre of this epidemic.
….All districts of Sierra Leone except one have recorded cases of Ebola, but the hardest hit are the districts of Kenema and Kailahun. Kenema is the third largest city in Sierra Leone, and the centre of the country’s lucrative diamond trade, while Kailahun is a major regional hub. The first recorded case in Sierra Leone was confirmed in Kailahun, and to date, there have there have been 570 confirmed Ebola cases in these two districts alone. This is epicenter of Ebola in Sierra Leone, and as of this morning, the districts of Kenema and Kailahun, with a combined population of over 950,000, are effectively locked down. Blockades on the major highways are ensuring that no one leaves or enters.
…“No one can leave Kenema,”…
…the ramifications are already being felt. The price of rice, an essential food in Sierra Leone, has already increased by 30 percent today alone. In the central market, the price of salt has doubled in the last 24 hours. …
edit on 8/8/14 by soficrow because: (no reason given)
a reply to: marg6043
There are trillions of dollars to be had by depopulating West Africa to clear the path for mining and "resource extraction" - but I'll give you that letting the virus "escape" means big bucks for Big Pharma. Guess they had to share the wealth. Or maybe the escape really was accidental. Either way, it's a big win.
There are trillions of dollars to be had by depopulating West Africa to clear the path for mining and "resource extraction" - but I'll give you that letting the virus "escape" means big bucks for Big Pharma. Guess they had to share the wealth. Or maybe the escape really was accidental. Either way, it's a big win.
a reply to: soficrow
Help me understand what that means? What does Nigeria's Irrua Specialist Teaching Hospital have to do with the outbreak in Nigeria?
I'm in several ebola threads, maybe I missed something?
originally posted by: soficrow
Sawyer is being blamed for bringing Ebola to Nigeria but I call bs - it started in Nigeria's Irrua Specialist Teaching Hospital with the 'research' arm.
Help me understand what that means? What does Nigeria's Irrua Specialist Teaching Hospital have to do with the outbreak in Nigeria?
I'm in several ebola threads, maybe I missed something?
edit on 8-8-2014 by loam because: (no reason given)
originally posted by: loam
.....What does Nigeria's Irrua Specialist Teaching Hospital have to do with the outbreak in Nigeria?
I'm in several ebola threads, maybe I missed something?
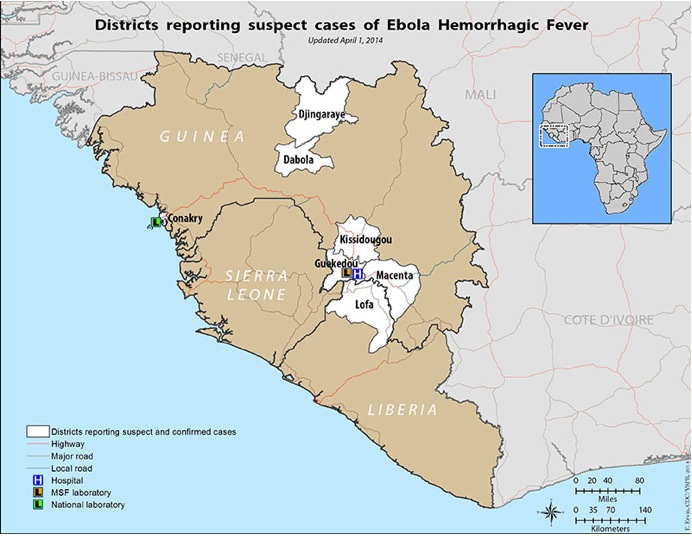
I call bs on the whole "Blame Sawyer" strategy. The US consortium [VHFC] was experimenting with viral hemorrhagic fevers in Nigeria at Irrua Specialist Teaching Hospital and the University of Lagos - not just Kenema Hospital at the epicenter in Sierra Leone, Guinea and Liberia. The really cool thing? No ethics review or oversight. And in case you missed it, check out the acknowledged epicenter in the map below - and note the big blue "H" denoting hospital. Oh yeah, and check out these threads: US Biological Warfare Researchers in the Ebola Zone, and EBOLA: Clearing the Path for US Corporate Investments in Africa?.
Molecular Diagnostics for Lassa Fever at Irrua Specialist Teaching Hospital, Nigeria: Lessons Learnt from Two Years of Laboratory Operation
…….Only the laboratory at the hospital in Kenema, Sierra Leone, which has become operational since 2004 (after civil war forced its closure in 1993), is able to perform Lassa fever testing for patients [30]. In Nigeria, the situation improved with the implementation of Lassa virus PCR testing at a research laboratory of the University of Lagos ….
…….The diagnostic and research laboratory was built in 2008 and started operation in September 2008.
……..The study was classified as a service evaluation and granted exemption from ethical review by the Research and Ethics Committee of ISTH. …….Service evaluation is exempt from ethical review according to the National Code of Health Research Ethics, National Health Research Ethics Committee, Federal Ministry of Health, Nigeria.
April 1, 2014
UPDATE
Guinea shuts borders with Sierra Leone and Liberia
Guinea announced the closure of its borders with Sierra Leone and Liberia on Saturday in a bid to halt the spread of Ebola, a virus that has killed nearly 1,000 people in the three countries this year.
….Nigeria became the third African nation, after Sierra Leone and Liberia, to declare a national emergency on Friday as the region's healthcare systems struggle to cope with the advance of one of the deadliest diseases known to man.
Nigeria declares state of EMERGENCY as Guinea CLOSES borders
a reply to: soficrow
has a visual pie chart of final destinations.
theextinctionprotocol.wordpress.com...
has a visual pie chart of final destinations.
theextinctionprotocol.wordpress.com...
For this reason, spread within Africa is really what public health officials are worried about. “Our first concern is that this is going to go into adjacent areas through people traveling in the region,” said Daniel Bausch, associate professor at the Tulane University School of Public Health and Tropical Medicine, who is working with the WHO and MSF on the outbreak. “In the short term, the main vector is the traveler: local people traveling from one village to the next, on more regional scale, plane travelers.” This pie chart shows the final destinations of travelers originating in the three countries currently most affected by Ebola. As you can see, travel from Sierra Leone, Guinea and Liberia within the continent is much more prevalent than travel elsewhere. All countries in West Africa are already on alert. National authorities in Ghana, Nigeria, Togo and the Côte d’Ivoire are working with the WHO on prevention efforts and monitoring potential cases. To do this, contact tracing is essential, said Bausch.
a reply to: 727Sky
Great report. Thanks S&
...BUT. (Of course there's a but.) ...1. The analysis is based on observations of previous Ebola outbreaks but this is a new sub-clade that's acting quite differently. 2. The initial emergence in different areas, rapid spread and as well, what seem to be cover-ups in Sierra leone and Nigeria, strongly indicate a direct association with the 2 hospitals working with the US-led VHFC (in Kenema and Nigeria), involving the US Military and bio-defense corporations.
If this were Ebola-as-usual, the 'outbreak' would have ended back in December in the isolated village where the index patient lived. Instead, within 3 short months, it had spread from the hospital-center in Kenema throughout several adjacent regions. (See map below.) ...and the fact Nigeria declared a National Emergency with only one confirmed case on the books makes it obvious there's a whole lot going on there that they're not telling us. 'Cuz Nigeria's government is not exactly recognized for it's sense of responsibility.
Seems clear something went wrong, but who knows what? ...I don't think we'll ever be told.
April 1, 2014
From your source:
ETA NOTE: Your source is dead-on about the worst-case scenario - "the disease will continue to bubble on, like a persistent bushfire, never quite doused out. It may start to approach endemic status in some of the worst affected regions." Which is exactly what happened with H5N1 bird flu in Asia.
Great report. Thanks S&
...BUT. (Of course there's a but.) ...1. The analysis is based on observations of previous Ebola outbreaks but this is a new sub-clade that's acting quite differently. 2. The initial emergence in different areas, rapid spread and as well, what seem to be cover-ups in Sierra leone and Nigeria, strongly indicate a direct association with the 2 hospitals working with the US-led VHFC (in Kenema and Nigeria), involving the US Military and bio-defense corporations.
If this were Ebola-as-usual, the 'outbreak' would have ended back in December in the isolated village where the index patient lived. Instead, within 3 short months, it had spread from the hospital-center in Kenema throughout several adjacent regions. (See map below.) ...and the fact Nigeria declared a National Emergency with only one confirmed case on the books makes it obvious there's a whole lot going on there that they're not telling us. 'Cuz Nigeria's government is not exactly recognized for it's sense of responsibility.
Seems clear something went wrong, but who knows what? ...I don't think we'll ever be told.
April 1, 2014
From your source:
...“With Ebola outbreaks, most of the time there’s one or very few introductions of the virus from the wild into humans, and all the transmission after that is human-to-human transmission. So people who are traveling locally as well as on planes and other modes of transport, that’s the way this would get around.”
....“The worst-case scenario is that the disease will continue to bubble on, like a persistent bushfire, never quite doused out,” said Derek Gatherer, a Lancaster University bio-informatician who has studied the evolution of this Ebola outbreak. “It may start to approach endemic status in some of the worst affected regions. This would have very debilitating effects on the economies of the affected countries and West Africa in general.”
This dire situation could come about because of a “persistent failure of current efforts,” he added. “Previous successful eradications of Ebola outbreaks have been via swamping the areas with medical staff and essentially cutting the transmission chains. Doing that here is going to be very difficult and expensive. We have little option other than to pump in resources and engage with the problem using the tried-and-tested strategy—but on a scale previously unused.”
ETA NOTE: Your source is dead-on about the worst-case scenario - "the disease will continue to bubble on, like a persistent bushfire, never quite doused out. It may start to approach endemic status in some of the worst affected regions." Which is exactly what happened with H5N1 bird flu in Asia.
edit on 9/8/14 by soficrow because: (no reason given)
a reply to: soficrow
Maybe not a new subclade, but an evolved form of the older ZEBOV:
And why would seem so different?
Phylogenetic Analysis of Guinea 2014 EBOV Ebolavirus Outbreak
So since the virus has had more time to evolve (it has drifted 3% from its original sequencing), it's had more time to become more efficient at survival, or has had help.
Now, the fact that the virus shows signs of having recombined with older versions of itself may indicate that some monkey business has occurred.
Maybe not a new subclade, but an evolved form of the older ZEBOV:
This approach indicates that the outbreak in Guinea is likely caused by a Zaire ebolavirus lineage that has spread from Central Africa into Guinea and West Africa in recent decades, and does not represent the emergence of a divergent and endemic virus.
As the GP sequences show, without more diverse sequences, especially those from the animal reservoir, it is difficult to narrow down the estimates of when and through what means the Central African EBOV lineage has been introduced into West Africa.
And why would seem so different?
The branch leading to the Guinea outbreak is long, not because it is a divergent lineage but because it is the most recently sampled so has had the most time to evolve.
Phylogenetic Analysis of Guinea 2014 EBOV Ebolavirus Outbreak
So since the virus has had more time to evolve (it has drifted 3% from its original sequencing), it's had more time to become more efficient at survival, or has had help.
Now, the fact that the virus shows signs of having recombined with older versions of itself may indicate that some monkey business has occurred.
originally posted by: jadedANDcynical
a reply to: soficrow
Maybe not a new subclade, but an evolved form of the older ZEBOV:
Isn't that just the simple explanation of what a subclade is?
Novel Zaire Ebola Sub-Clade In Guinea and Sierra Leone
All 101 sequences form a Zaire sub-clade which signals clonal expansion due to human to human transmission following a single introduction. These 101 sequences are easily distinguished from all other Zaire sub-clades, which have been associated with the largest number of reported Ebola outbreaks, including the previously most deadly outbreak in Yambuku, Zaire in 1976 (280 deaths in 318 cases), which was followed by the second most deadly outbreak, which was 19 years later in Kikwit, Zaire in 1995 (245 deaths in 317cases).
Full-length genome sequencing and phylogenetic analysis showed that EBOV from Guinea forms a separate clade in relationship to the known EBOV strains from the Democratic Republic of Congo and Gabon.
a reply to: soficrow
UPDATE
Bravo Guinea. Just to recap:
UPDATE
Guinea has NOT closed its borders.
Bravo Guinea. Just to recap:
1) quarantine has been historically used to discriminate against minorities;
2) studies demonstrate that mass quarantine is ineffective;
3) a large scale quarantine would be difficult to implement.
An outbreak should meet the following three criteria for quarantine to be a useful measure of disease control:
* people likely to be incubating the infection must be efficiently and effectively identified;
* those people must comply with the conditions of quarantine; and
* the infectious disease in question must be transmissible in its presymptomatic or early symptomatic stages.
The use of quarantine in the Toronto (SARS) outbreak failed on all three counts.
Ebola virus: Liberia health system 'falling apart'
….The MSF co-ordinator in Liberia said official figures were "under-representing the reality", and that the health system was "falling apart".
…Meanwhile, neighbouring Guinea has denied earlier reports that it had sealed its borders.
…In Guinea, the health minister on Saturday said the borders with Liberia and Sierra Leone had been closed to prevent infected people crossing into the country.
However, state television later said: "Guinea has not closed its borders with Sierra Leone or with Liberia. It's rather that we have taken health measures at the border posts."
A government source told Reuters that the minister who made the original announcement had not been in possession of accurate information.
Nigeria is declaring more cases. I'm thinkin' there's a whole lot more than they're admitting.
Nigeria Struggles to Cope With Ebola Outbreak
Nigerian health officials have announced 10 confirmed cases and two deaths in the country from the Ebola outbreak that is sweeping West Africa, including a nurse and a man from Liberia whom the nurse had been caring for.
…“Rapid epidemic transmission has been with us a long time, but my guess is that it’s accelerating, with the number of people on the move and intensity of air travel, global trade and the numbers of displaced people we have globally,” said Jeffrey D. Sachs, an economist and the director of the Earth Institute at Columbia University.
Climate change, population growth and an increase in displaced populations mean that people are pushing into previously uninhabited places, creating new vulnerabilities and bringing humans into closer contact with animal populations, where many of the diseases have begun, he said.
….At the same time, globalization means that people are mixing more, trading more and handling more farm animals in industrial settings — all of which facilitate the emergence and spread of infectious diseases.
“This ought to force a reflection,” Mr. Sachs said, adding that establishing a basic network of community health workers across the developing world was an urgent priority.
a reply to: soficrow
Interesting note about the nurse. She claims to have not come in contact with his body fluids.
Another interesting note is that Patient Zero is reported to be a 2 year old boy, which raises interesting questions about how the infection started. Hmmmm.
Link.
Interesting note about the nurse. She claims to have not come in contact with his body fluids.
One of those Nigerian health care workers, Obi Justina Ejelonu, who was on duty at the First Consultant Hospital in Obalende, Lagos when Sawyer was brought in, is said to be clinging onto her life after contracting the virus. Ironically, Obi Justina had initially posted a message on her Facebook page boasting that she had limited contact with Sawyer and was grateful to God to be alive:
Obi Justina wrote: “I never contacted his fluids. I checked his vitals, helped him with his food (he was too weak)…..I basically touched where his hands touched and that’s the only contact. Not directly with his fluids. At a stage, he yanked off his infusion and we had blood everywhere on his bed…..but the ward maids took care of that and changed his linens with great precaution.”
Link.
Another interesting note is that Patient Zero is reported to be a 2 year old boy, which raises interesting questions about how the infection started. Hmmmm.
Link.
edit on 11-8-2014 by loam because: (no reason given)
a reply to: soficrow
I don't think so. The paper I've quote references the work you've sourced and indicates that the initial analysis may be wrong:
I think if it were different in the way Blaize et al are implying, it would be on a different branch than in this graph:
Phylogenetic Analysis of Guinea 2014 EBOV Ebolavirus Outbreak
If this were a different enough variant, it would probably be called Guinea Ebola Virus (GEBOV), but this is clearly THE ZEBOV from the central African outbreaks of the 70s.
Isn't that just the simple explanation of what a subclade is?
I don't think so. The paper I've quote references the work you've sourced and indicates that the initial analysis may be wrong:
We believe that at present no suitable outgroup sequences to root the EBOV phylogeny exist and that a temporal rooting gives the most consistent results.
This approach indicates that the outbreak in Guinea is likely caused by a Zaire ebolavirus lineage that has spread from Central Africa into Guinea and West Africa in recent decades, and does not represent the emergence of a divergent and endemic virus.
As the GP sequences show, without more diverse sequences, especially those from the animal reservoir, it is difficult to narrow down the estimates of when and through what means the Central African EBOV lineage has been introduced into West Africa.
I think if it were different in the way Blaize et al are implying, it would be on a different branch than in this graph:
Phylogenetic Analysis of Guinea 2014 EBOV Ebolavirus Outbreak
If this were a different enough variant, it would probably be called Guinea Ebola Virus (GEBOV), but this is clearly THE ZEBOV from the central African outbreaks of the 70s.
new topics
-
Plane Crash in South Korea
Mainstream News: 7 hours ago -
Cutting Boards
Food and Cooking: 10 hours ago -
Mexico Plans Alert App For Migrants Facing Arrest In US
Mainstream News: 11 hours ago
top topics
-
Why Such An Uproar Over Non-US Citizens With H1-B Work Visas.
Social Issues and Civil Unrest: 16 hours ago, 8 flags -
Cutting Boards
Food and Cooking: 10 hours ago, 7 flags -
Mexico Plans Alert App For Migrants Facing Arrest In US
Mainstream News: 11 hours ago, 6 flags -
Plane Crash in South Korea
Mainstream News: 7 hours ago, 5 flags
active topics
-
New York Governor signs Climate Law that Fines Fossil Fuel Companies
US Political Madness • 33 • : Lazy88 -
UK Borders are NOT Secure!
Social Issues and Civil Unrest • 17 • : gortex -
Petition Calling for General Election at 564,016 and rising Fast
Political Issues • 175 • : gortex -
New UK Petition - Close the borders! Suspend ALL immigration for 5 years!
Regional Politics • 8 • : angelchemuel -
Cutting Boards
Food and Cooking • 4 • : angelchemuel -
Plane Crash in South Korea
Mainstream News • 5 • : Springbok -
Christmas Car Near Detroit…
Automotive Discussion • 9 • : JJproductions -
Mood Music Part VI
Music • 3769 • : paviabari -
Why Such An Uproar Over Non-US Citizens With H1-B Work Visas.
Social Issues and Civil Unrest • 44 • : WeMustCare -
-@TH3WH17ERABB17- -Q- ---TIME TO SHOW THE WORLD--- -Part- --44--
Dissecting Disinformation • 3837 • : brewtiger123